
Orthopedics- Upper extremity #3 discussion
Posted on: April 2, 2019, by : Jennifer Chapman
Jennifer Chapman, MD Children’s National Medical Center
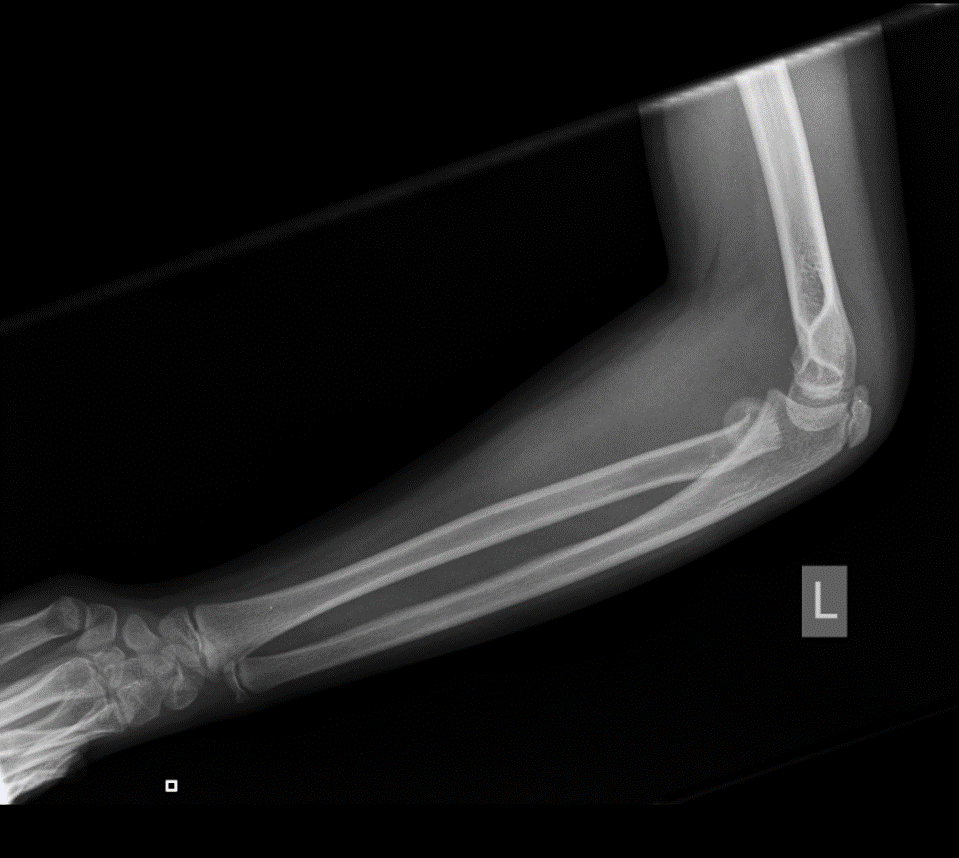
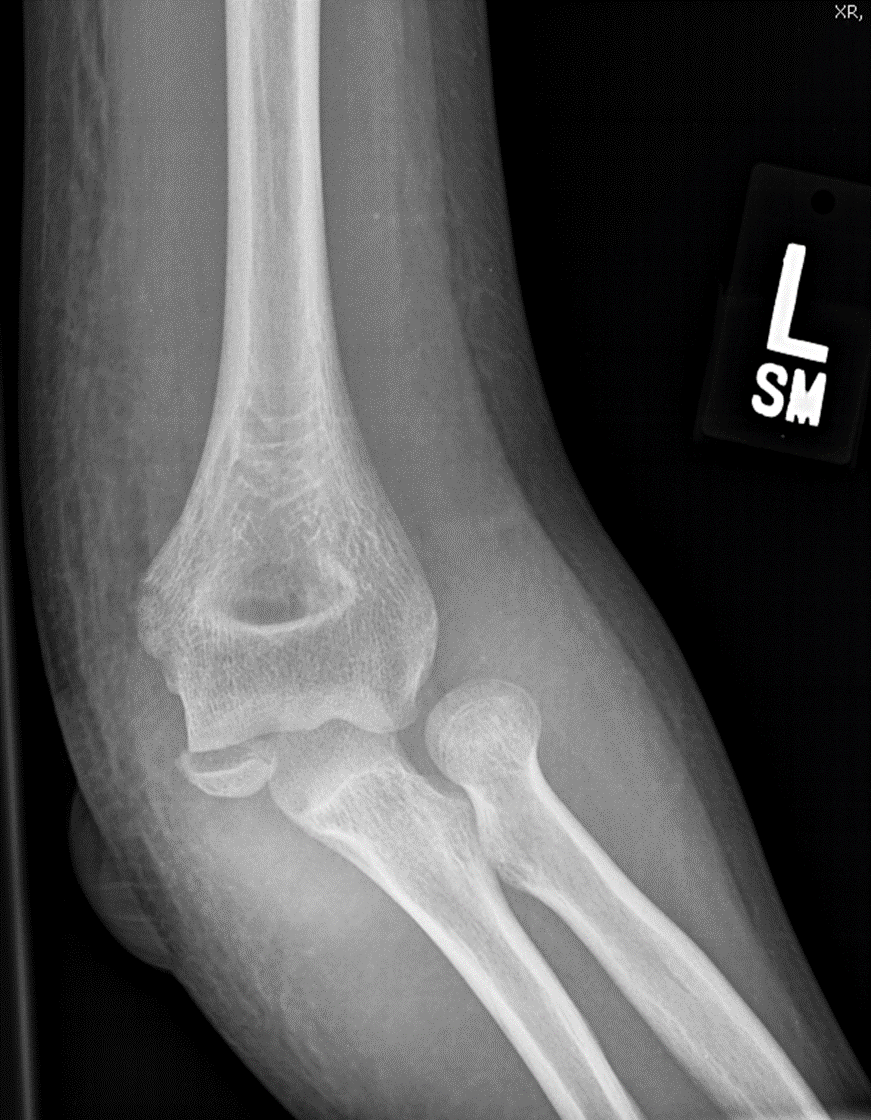
This 10 yo boy fell back onto his hand and has elbow pain and swelling, with limited pronation/supination.
There were 17 respondents, with injuries described as:
Elbow effusion Type 1 SCFx 7 40%
Lateral condyle fracture 6 35%
Radial neck fracture 4 25%
Other, describe: —
Diagnosis: fracture of radial neck
Our Orthopedic colleague responds:
Treatment: well-padded long arm posterior splint just past the wrist. The splint MUST prevent pronosupination. For non-displaced fractures, a 7-10 day follow-up is appropriate. For displaced/surgical fractures, the follow-up is sooner (ED consult or outpatient follow-up within 1-2 days).
Clinical Pearls:
1.On clinical exam, pain may be greater with gentle passive pronosupination of the forearm than with flexion and extension of the elbow. Pain can be referred to the wrist but the child will have tenderness over the radial head.
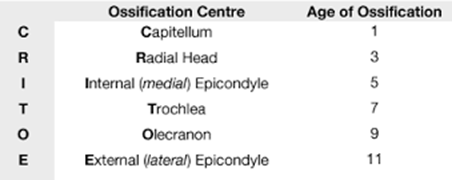
2. Xray: based on CRITOE, the ossification centers indicate an 11yo. In the previous discussion, I posted the 1, 3, 5, 7, 9, 11 rule for the age at which the sequential ossification centers come in. The learning point is that CRITOE is reliable in terms of the ORDER in which the ossification centers appear, but not perfectly so for the actual age.
3. What is CRITOE again?

4. The AP view of the elbow is typically focused on the distal humerus. If there is a radial neck fracture and you can’t see sufficiently to measure angulation/displacement, order an AP elbow with attention to proximal radius/ulna. This is entered under comments in the EMR.
5.When an elbow effusion is present, examine all the bones within the joint capsule for a fracture.
6.The radial head should point towards the capitellum on all x-ray views.
7.Even fractures that heal anatomically can result in some loss of elbow or forearm motion.
Red flags requiring Orthopedic consult in the ED:
1.angulation is difficult to quantify on x-ray, but can be improved with the technique describe in #4 above. Any angulation or displacement should be evaluated by orthopedic surgery*. Surgical considerations for the orthopedic surgeon are >2mm displacement and >20 degrees angulation.
2. look for associated injuries – elbow dislocation (= radial head does not point to the capitellum), ulna fracture with or without dislocation (with dislocation is a Monteggia fracture), medial epicondyle fracture or other fracture patterns.
3.associated nerve palsy or an open fracture require consultation.
*this is true at most academic institutions where the ED-ortho relationship is robust. There are other approaches possible when EDs have mechanisms in place for treating non-emergent but operative fractures– relationships with Orthopedic surgeons that allow scheduling of outpatient surgery soon after ED visit.
Pattern recognition:










Injuries seen:
Case 2: radial neck fracture with joint effusion.
Case 3: radial neck fracture and joint effusion
Case 4: medial epicondyle fracture, with fracture fragment trapped in joint. The post-op hardware points to the injured bone:

Case 5: radial neck fracture with effusion.
Case 6: radial neck fracture and joint effusion. The next image is an arthrogram in a same-aged child. It shows how large the fracture fragment is, as there is unossified portions that are not visible on xray.

Case 7: type 1 supracondylar fracture (SCFx)
What remains unclear?