
Pediatric Elbow
Posted on: August 16, 2020, by : Haroon Shaukat MDSupracondylar
Introduction:
- One of the most common pediatric fractures seen, mechanism tends to be fall on an outstretched hand
- extension type most common (95-98%)
- flexion type less common (<5%)
- When reviewing x-rays of the elbows, consider ossification/appearance and age of fusion (two independent events)
- C-R-I-T-O-E mnemonic to remember age of ossification
| Ossification center | Years at ossification (appear on xray) (1) | Years at fusion (appear on xray) (1) |
| Capitellum | 1 | 12 |
| Radial Head | 4 | 15 |
| Internal (Medial) epicondyle | 6 | 16-18 |
| Trochlea | 8 | 12 |
| Olecranon | 10 | 16 |
| External (Lateral) epicondyle | 12 | 12 |
| (1) +/- one year, varies between boys and girl |
Classification:
- Type 1: Non-displaced (posterior fat pad sign on lateral view of x-ray)
- Treated with posterior long arm splint in ED
- Urgent Orthopedics follow up for cast immobilization x 3-4 weeks
- Type 2: Displaced (“hinge” fracture with posterior cortex intact)
- Treated with cast immobilization in the ED
- Urgent Orthopedics follow up radiographs in 1-2 weeks
- Type 3: Completely displaced (+/- distraction)
- Treated with closed reduction and percutaneous pinning by orthopedics
- Non-emergent (overnight) operation unless neurovascular compromise
Complications:
- Vascular compromise (<20%)
- often maintains circulation secondary to rich collateral supply
- Associated distal radius fracture
- consider routine forearm x-rays with elbow pathology
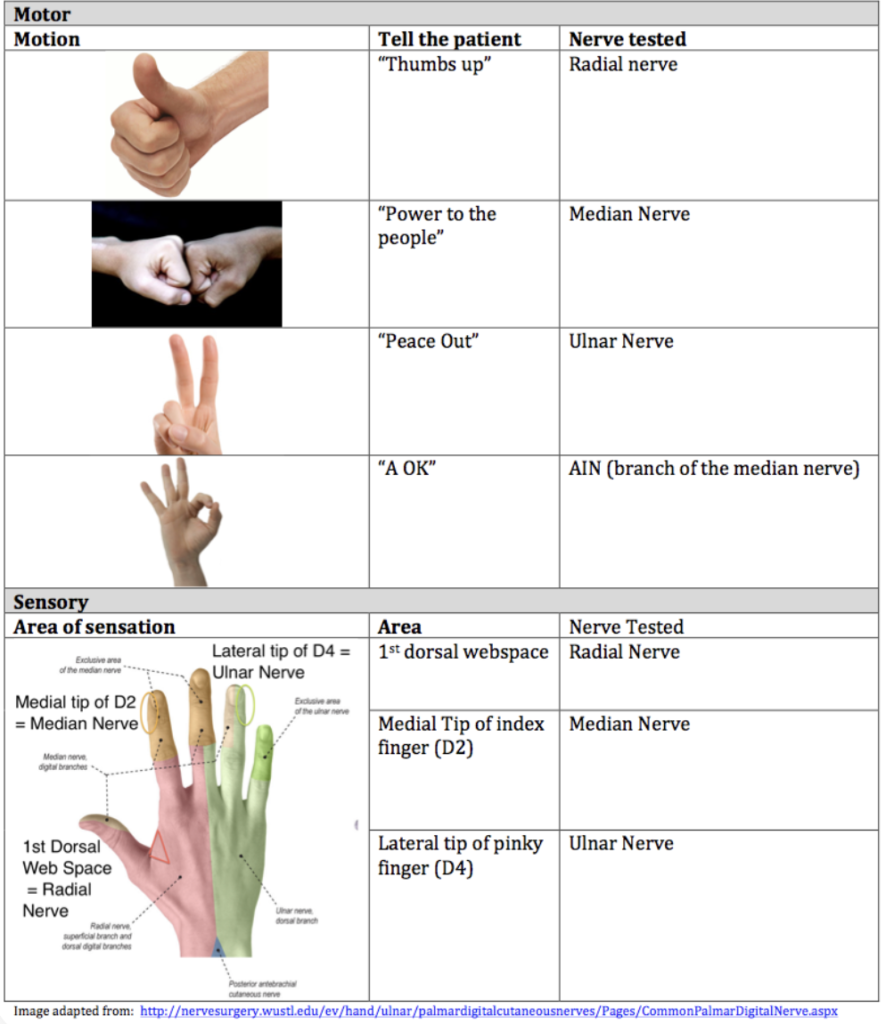
- Anterior interosseous nerve (AIN) neuropraxia (most common)
- unable to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger (can’t make A-OK sign)
- Radial nerve neuropraxia (second most common)
-
- inability to extend wrist, MCP joints, thumb IP joint
-
- Median nerve neuropraxia
-
-
- loss of sensation over volar index finger
-
-
- Ulnar nerve neuropraxia (tends to be flexion-type injuries)
Lateral Condyle
Introduction:
- Second most common fracture in the pediatric elbow and are characterized by a higher risk of nonunion, malunion, and avascular-necrosis than other pediatric elbow fractures.
- <20% of all pediatric distal humerus fractures
- “Pull-off” mechanism: avulsion fracture from the pull of the common extensor musculature
- “Push-off” mechanism: fall onto an outstretched hand causes impaction of radial head to the lateral condyle
- When reviewing x-rays of the elbows, consider ossification/appearance and age of fusion (two independent events)
- last ossification center to appear (around 12 years of age)
- need internal oblique view (fracture is posterolateral)
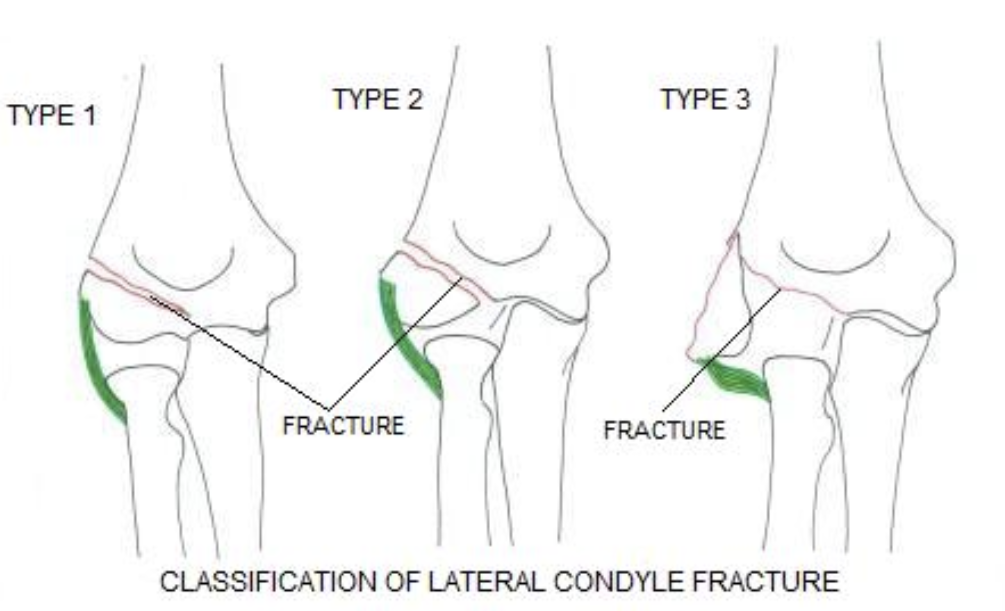
Classification:
- Type 1: <2 mm fracture displacement
- Treated with cast immobilization in the ED
- Urgent orthopedics follow up in 1 week for radiographs
- Type 2: Between 2 and 4 mm fracture displacement
- Treated with closed reduction and fixation
- Type 3: >4 mm fracture displacement
- Treated with open reduction and fixation
Complications:
- Stiffness (most common complication)
- can be a early sign of non-union or delayed union
- Nonunion (higher incidence than other elbow fractures)
- risk factors include nonsurgical management
- AVN (occurs up to three years after fracture)
- risk factors include posterior dissection
- Lateral overgrowth/prominence
- up to 50% regardless of treatment
- spurring is correlated with greater initial fracture displacement
Medial Condyle
Introduction:
- Third most common fracture in the pediatric elbow and are increasing in incidence due to increased athletic demands of children
- 75% occur in boys between 9-14 years old
- Avulsion mechanism: avulsion fracture from the pull of the ulnar collateral ligament
- Direct trauma
- 50-60% associated with elbow dislocations
- When reviewing x-rays of the elbows, consider ossification/appearance and age of fusion (two independent events)
- last and final ossification center to fuse (around 16 years of age)
- need internal oblique view
Classification:
- Acute
- Nondisplaced, displaced, or fragment entrapped in joint
- Chronic
- related to tension stress injuries
- Treatment is nonoperative with cast immobilization
- ORIF if displacement with entrapment of medial epicondyle fragment in joint
Complications:
- Stiffness (most common complication)
- Nonunion (majority are asymptomatic)
- Neuropraxia/Nerve Injury (ulnar nerve)
Alternative Diagnosis:
- Little League Elbow (medial epicondyle stress fracture)
- Risk factors include: >80 pitches per game, >8 months of competitive pitching per year, Fastball speed >85 mph
- Pain with valgus stress and tenderness to palpation of medial elbow
- Treatment is rest, activity modifications, and physical therapy
Olecranon
Introduction:
- Uncommon fracture of children
- <5% of all pediatric fractures
- FOOSH mechanism with elbow in flexion OR extension
- Direct trauma mechanism
- Olecranon avulsion fractures are highly suspicious for Osteogenesis Imperfecta
- When reviewing x-rays of the elbows, consider ossification/appearance and age of fusion (two independent events)
- fusion of the olecranon occurs from anterior to posterior
- partial closure may be mistaken for olecranon fracture
Classification:
- Acute
- Nondisplaced
- Chronic
- related to tension stress injuries
- Treatment is nonoperative with cast immobilization
- ORIF if displacement or unstable fracture
Complications:
- Stiffness (most common complication)
- Nonunion
- Delayed union
- Neuropraxia (ulnar nerve)
| Other Helpful Resources |