Hot Seat #159: 11 yo F with altered mental status
Posted on: October 15, 2020, by : Mary Beth Howard
Jonathan Lee, MD, Inova Fairfax Children’s Hospital
HPI: 11 year old female with medical history significant for headaches and anxiety, presenting with concerns for brief alteration in mental status. Two hours prior to presentation, Patient finished watching a movie with her family and was told to get ready for bed. Per Mother, patient did not respond and appeared to be staring off.
Mom repeated herself, and patient got up, as if to go upstairs, but instead, walked past the stairs and went to her father who was on the phone. Patient was given the phone, but did not speak. Patient states she felt “blurry,” and that she had trouble finding words to speak. Mom states that she noted the patient was acting weird, not responding, and appeared to be getting anxious. This episode lasted 10 minutes. Patient does not remember all of the event, but remembers trying to speak with grandmother. Spoke with on call PCP who referred to emergency room. There were no jerking or other abnormal movements. She had headache earlier in the day, but by time of episode, had resolved. She has a history of mild intermittent headaches. Was evaluated by PCP and advised to use PRN OTC medications.
Per Mom, has anxiety, is not on medications.
Patient denied taking any other medications that day. Denied drug use, SI, HI. She feels safe at home.
PMH: Headaches and Anxiety
Medications: None
ROS: Denied fever, cough, nausea, vomiting, fall, head trauma
Exam:
Pulse 106 | BP 124/74 | Resp 16 | SpO2 98 % | Temp 99.2 °F (37.3 °C) | Wt 36.9 kg
GENERAL APPEARANCE: Sitting in ED bed without distress. Conversive and friendly.
SKIN: No bruising
HEAD: Normocephalic. Atraumatic.
EYES: PERRL. EOMI. No conjunctival injection or discharge noted.
EARS: Bilateral Tympanic membranes were clear, not bulging, or erythematous.
NT: MMM, no posterior pharyngeal erythema noted.
NECK: Supple with good range of motion.
LUNGS: Clear to auscultation bilaterally. No wheezes, rhonchi, rales. No increased WOB.
CARDIOVASCULAR: There was a regular rate and rhythm without any murmurs
ABDOMEN: Soft, nontender, non distended
MUSCULOSKELETAL: Moves all extremities.
NEUROLOGIC: Alert and appropriate, answers questions appropriately. Baseline mentation. PERRL. EOMI. Facial sensation in V1 – V3 intact bilaterally. Smile and eye closure appear symmetric. No tongue deviation or fasciculations noted, able to move it side to side. Uvula appears midline with saying AH. Shoulder shrug with good strength. Head turn with good strength. Biceps/triceps/hand strength 5/5. Quad/hamstring strength 5/5. Patellar reflex 2+. Coordination intact on finger to nose to full extension bilaterally. Gait appears normal. Speech appears normal.
Head CT:
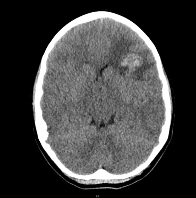
FINDINGS: There is a lobulated area of increased density within the subcortical and deep white matter of the anterior left frontal lobe at the level of the lateral ventricles measuring approximately 2.2 cm x 2.2 cm axial dimensions consistent with hemorrhage. There is moderate surrounding vasogenic edema that causes partial effacement of the left lateral and third ventricles. Midline shift to the right measures 2-3 mm. The basal cisterns are patent. There is a small left maxillary sinus retention cyst. The middle ear cavities and mastoid air cells appear clear.
Radiology is prepared to take patient immediately back for any additional imaging if needed.
The patient is endorsing the beginning of a very mild headache.
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.