Hot Seat #219: Denouement
Posted on: December 4, 2023, by : Brandon Ho
This week we highlight the case of a well-appearing child who presents with intermittent bilious emesis. The crux of the decision centered around the appropriate imaging when there is concern about malrotation with volvulus but an upper GI is unavailable.
Junior learners preferred a CT abdomen with contrast whereas senior learners preferred an abdominal ultrasound. All stressed the importance of timely imaging as bowel necrosis can occur quickly if a volvulus is left untreated. Both imaging modalities can diagnose obstruction however, ultrasound is faster and does not expose the patient to radiation. Ultrasound is more specific and sensitive for the diagnosis of volvulus than malrotation. If the US is positive for volvulus, the patient should be taken directly to surgery without further imaging. If the diagnosis is not clear, a limited upper GI series to view the duodenum. On the other hand, a normal US does not exclude malrotation.
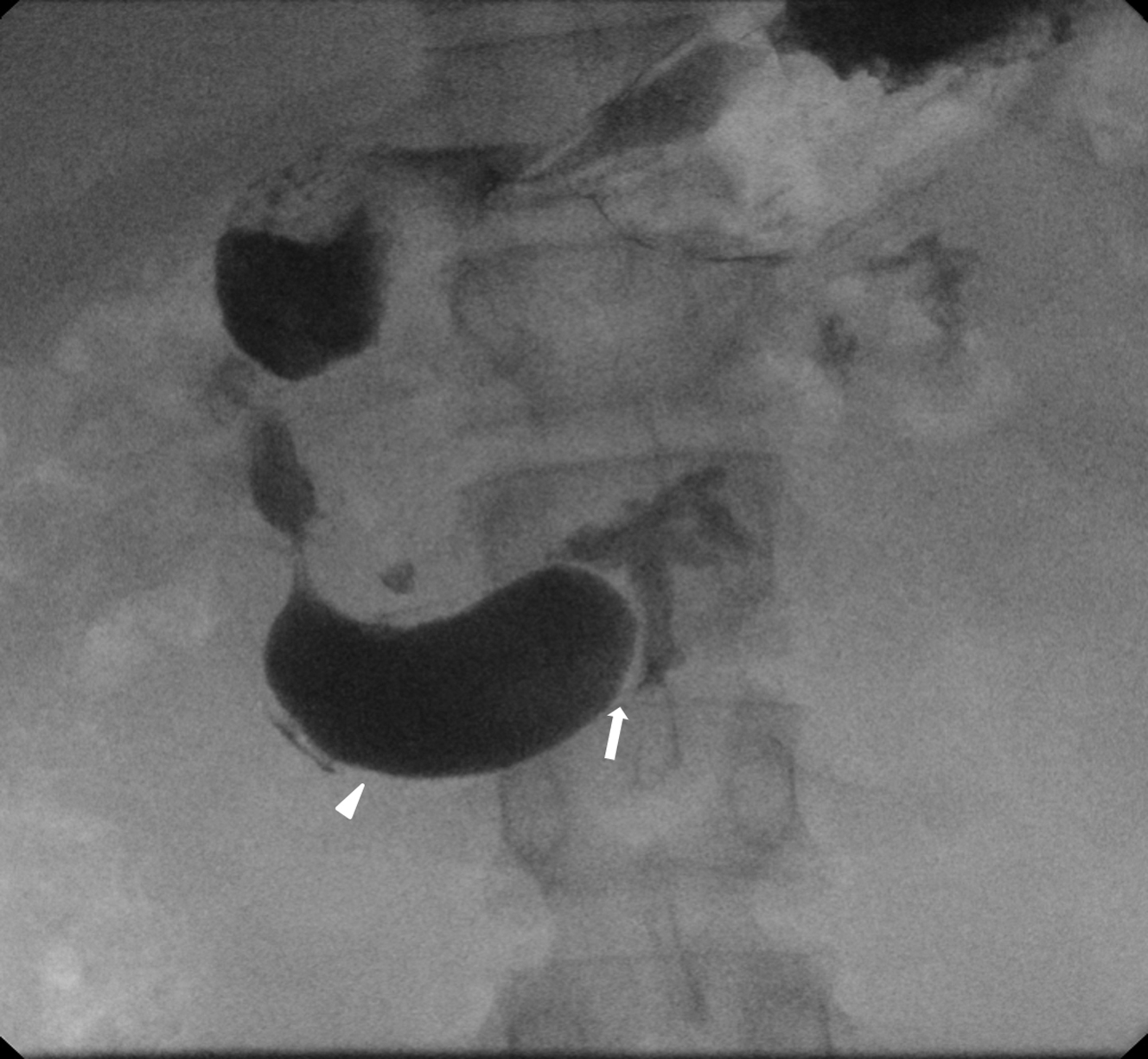
After much back and forth between surgery, hospitalist, and radiology, radiology agreed to come in to perform upper GI. Upper GI was performed which showed distention of the stomach and proximal duodenum with abrupt focal narrowing in the region of the proximal/mid duodenum concerning for a high-grade bowel obstruction. Differential included malrotation, annular pancreas, pre-duodenal portal vein. The patient was taken immediately to the OR where she was found to have a dilated proximal duodenum secondary to a duodenal web. She underwent a duodenoduodenostomy and was discharged on POD5 after an uncomplicated hospital course.
A duodenal web occurs when a membranous web in the duodenal lumen causes partial or intermittent obstruction. Radiographically, it can appear similar to duodenal atresia, but distal bowel gas usually is present. Typically upper GI will show a partial obstruction with a windsock deformity, which consists of an intraduodenal contrast-filled sac that is surrounded by a narrow lucent line as the barium in the duodenum passes distal to the web.