
Hot Seat #249: I Think I Need A Boost
Posted on: October 14, 2025, by : Brittany Fitzpatrick
Case by Jessica Williams, CNH PEM Fellow
15 yo presenting ~ 1 hour after low-speed MVC (10-15 mph). Improperly restrained passenger in back passenger side (belted but not in booster seat, pt is 20 kg). The car was hit on the back driver’s side and airbags were deployed. No LOC but had a few episodes of NBNB emesis (ate 30 min before the accident). Arrived POV complaining of abdominal pain.
PMH: mitral valve stenosis, bicuspid aortic valve with stenosis, transverse arch hypoplasia and aortic coarctation s/p repair, chronic lung disease
Vitals: 98% on RA, T 36.8C, HR 92, RR 22, no BP
Physical Exam
General: Alert, withdrawn
Skin: warm, intact
Head: atraumatic
Neck: supple, trachea midline, no tenderness
ENMT: oral mucosa moist
Cardiovascular: regular rate and rhythm
Respiratory: lungs are clear to auscultation, respirations are non-labored
GI: soft, generalized tenderness to palpation
MSK: moves all extremities.
Back: nontender
Neurologic: GCS 15
Ibuprofen is given, and the patient is observed to see if he tolerates PO. After a few hours, you decide to order basic trauma labs while you wait.
About 5 hours after patient arrival, labs are still pending, but family states that the patient is more sleepy than normal, which usually happens when he has heart issues. You try to wake him, but he is tired. He has tenderness to light palpation of his abdomen and is guarding. Mom tried to give him water but he threw it up. He also refused the previously ordered Motrin.
Labs:
Hgb 10.2, ALT 21, AST 42
Lipase 118 (Normal Range 10-69)
UA – still needs to pee!
Motrin was re-attempted but failed due to emesis so was given IV Zofran. Patient reported he needed to urinate and when he stood up in the bed he collapsed back down and went to sleep before he could try.
Head CT and Abd CT ordered.
Oh! And we finally got urine and the UA comes back!
urine spec grav 1.059
urine glucose neg
urine bilirubin neg
urine ketones 1+
urine blood neg
urine total protein 1+
urine urobilinogen normal
urine nitrite neg
urine leukocyte esterase neg
urine WBC none
urine RBC 6
urine bacteria none
As we wait, a lovely US fellow comes around looking for people to scan…

He finally goes for imaging:
Head CT neg
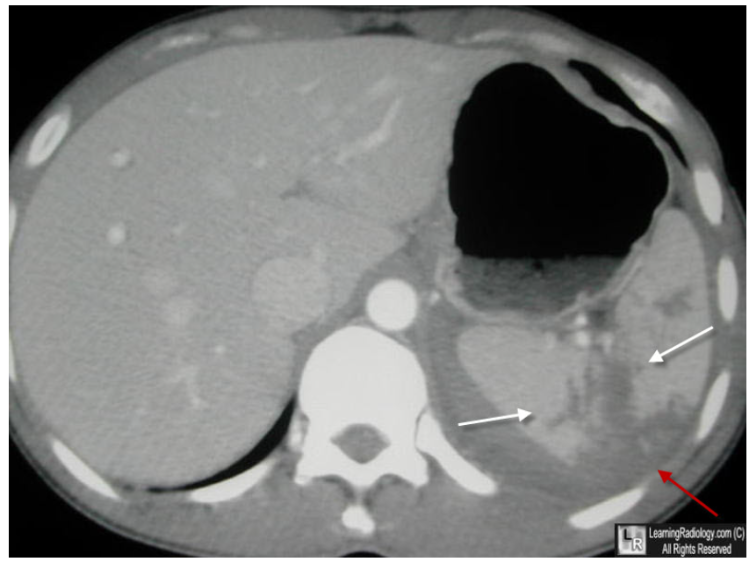
CT abd/pelvis impression:
1. High-grade splenic injury/devascularization (AAST grade IV-V) with large volume hemoperitoneum. No evidence of active extravasation or pseudoaneurysm.
2. Hyperattenuating adrenal glands and mild flattening of the IVC, which can be seen in the setting of CT hypoperfusion complex.
3. No pneumoperitoneum or acute osseous abnormality.
Trauma surgery consulted.
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.
Was that urine obtained in real time after the CT with IV contrast? It’s physiologically impossible for our kidneys to generate a specific gravity of 1.059! Spec gravs that high are usually secondary to IV contrast.
I think a big take-away from this case is to trust the exam! A trauma patient with abdominal pain and guarding needs more workup even if the labs are reassuring. I think this also speaks to the need for multiple reassessments of trauma patients for both mental status and injuries/tenderness that may have been missed or changed after our initial exams.
I think this case speaks to the importance of trusting our exams! In a trauma patient with abdominal pain and guarding, additional workup is crucial despite reassuring labs. Also speaks to the need for multiple reassessments as changes in mental status, pain and hemodynamics can change rapidly.