Hot Seat #259: It all falls down
Posted on: May 21, 2026, by : Brittany Fitzpatrick
Case by Kate Ritter, CNH PEM Fellow
Patient is a 17 y/o F otherwise healthy presenting via EMS from urgent care for having multiple episodes of syncope and lightheadedness today. She presented to urgent care today, and while in the clinic, pt states she fainted ~4x, but at least 8x total throughout the day today. Glucose was normal at UC. She describes the feeling as going limp and then falling and losing consciousness. Not associated with exertion. She feels “floppy” during these episodes. They last a few seconds. She is now experiencing generalized body shaking that started today. She currently feels generalized weakness and is unable to ambulate. Syncopal episodes are not preceded by prodromal vasovagal symptoms. Pt also states that she experiences shortness of breath before and after each syncopal episode. Does not have sleepiness or postictal phase after the episodes. She also reports 7-8/10 chest pain that feels like pressure, and the pain makes it hard to breathe is exacerbated by deep breaths. She has no prior history of chest pain, palpitations, or syncope prior to this week. No history of panic attacks. No fevers, URI sx, n/v/d, abdominal pain, headaches, dizziness, numbness or tingling. Pt is tolerating po well and reports no issues with UOP or BM. Denies taking any meds in an attempt to harm herself and has no past experiences of suicide attempts. Denies any recent drug use. Reports no current or recent stressors in her life or recent changes. No recent travel. Denies drug or alcohol use. IUTD. NKDA. No daily meds. Is currently on her menses. No OCPs or hormonal birth control.
Vital signs:
T 37.3 oral, HR 116, RR 25, BP 96/60, 97% on RA
Physical Exam:
General: Appears anxious and short of breath, taking quick shallow breaths and is diaphoretic but is able to be redirectable and is calm between these episodes.
HEENT: Normocephalic. PERRL. EOMI. Conjunctiva clear. Nares patent. Moist oral mucosa. No pharyngeal erythema.
Neck: Supple, full range of motion
Resp: Clear to auscultation bilaterally, respirations non labored, no tachypnea
CV: Tachycardic to 110s to 120s, orthostatic with increase in heart rate to 140s when sitting up. Regular rhythm. Normal S1, S2. No murmur appreciated.
GI: Soft, Nondistended, non-tender, normal BS
Integumentary: Warm, intact, no rash.
MSK: Unable to walk, falls over when attempting to ambulate
Neuro: Awake and alert and mentating normally, cranial nerves intact, extraocular movements normal, normal finger-to-nose. She has intermittent bilateral upper extremity jerking and shaking and tremulousness, movements are suppressible and patient is conscious during them. She has 3 out of 5 strength symmetrically in bilateral upper and lower extremities, able to resist against gravity but unable to resist examiner. When attempting to raise leg, the contralateral leg pushes into the bed. Her patellar reflexes are 2+ bilaterally and symmetric. No clonus.
Orthostatics were unable to be completed because patient had a “syncopal episode” witnessed by nursing but not witnessed by provider, in which patient slumped over and was briefly unresponsive after being transitioned from supine to sitting.
Other results:
WBC 7.31, Hb 14.6, HCT 43.7, platelets 242
Glucose 86
CMP normal
CK 101
TSH 1.23 (range 0.52 to 4.13)
D dimer 0.3 (normal <= 0.42)
Troponin < 4
UDS negative
UA with 66 RBCs, 13 squamous cells, rare bacteria, 3+ blood, 1+ ketones, otherwise negative
Upreg negative
CXR was negative
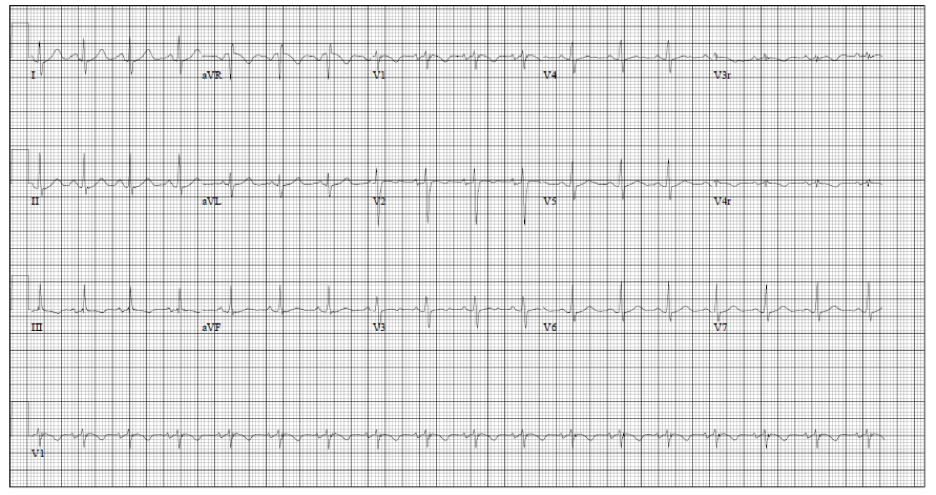
EKG shown
Patient remains tachycardic and has not had a HR below 100 while in the ED. She is still complaining of 7/10 chest pain, worse with deep breaths, subjective SOB but normal saturations, and feeling of generalized weakness.
Cardiology was consulted to review EKG given chest pain and episodes of LOC not preceded by prodromal vasovagal symptoms. During cardiology’s assessment, was noted to have tachypnea that resolved with reassurance. Was also found to have mild TTP over sternum. On their review of telemetry, sinus tachycardia and no arrhythmias seen, although significant artifact due to patients general tremulousness.
Patient remained unable to ambulate and still had 3/5 generalized weakness. Heart rate improved to low 100s after bolus.
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.