
Hot Seat #47 Denouement: 2 week old F w/ tachypnea and retractions
Posted on: November 21, 2014, by : Lenore Jarvis MD MEd
by Kaynan Doctor, Children’s National
with Desiree Seevaye, Children’s National
The Case
2 week old female presenting with her mother for tachypnea and retractions. This case offered a great discussion on work-up needed and disposition required (NICU vs floor vs home).
Here’s How You Answered Our Questions
#1: Other <3 yrs: review CXR w/ rads, ribs on right? EKG.
#1: Other >3 yrs: ECG, vbg, cards for echo. skeletal survey. cardiology consult and echo. O2 sat, radiology reading of CXR for c/f right sided rib fractures.
#2: Other >3yrs: ECHO. head CT.
As we have learned in the past, addressing ALTE (an apparent life-threatening event) is never easy. Many times it is sufficient not to do labs/imaging and make admission/observation the “treatment.” A thorough history and physical exam can help guide further testing. However, this patient had tachypnea (rapid breathing) and dyspnea (retractions/SOB), which is concerning for something more than an ALTE, so a CXR and further testing was done (below). Despite concerns for NAT, the CXR was unconcerning for fracture per Radiology. The majority of providers agreed that with RR 80 and retractions, admission is warranted. Some would admit to NICU (although an LP and sepsis workup might follow). Others would admit to the floor. Interestingly, this patient was admitted to the CICU.
Denouement
As the evening goes on, maternal grandmother phones in and mentions that her daughter presented the same way as a child and that she had some unusual heart rhythm that required electrical treatment using a wire from her leg. On further questioning you realize that Mom used to have Wolff-Parkinson-White syndrome that was successfully ablated as a child. An EKG is performed revealing the following:
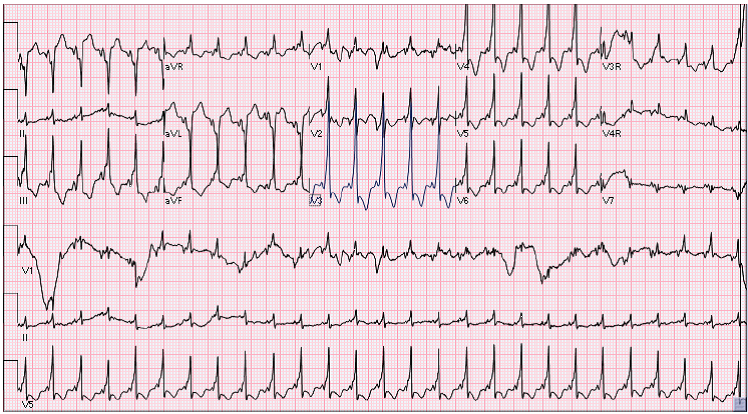
EKG: Sinus rhythm with short PR with suspected delta wave vs. right bundle branch block. Cardiology was consulted and performed a bedside echo which showed small muscular VSD, PFO w/left to right shunting, mildly decreased function, mild MR and EF of 46%. The patient was subsequently transferred to CICU for further care due to persistent tachypnea to 80s. During her CICU stay she had 3 episodes of SVT into the 280s that was controlled with adenosine and increasing doses of flecainide after which she was symptom free and discharged home on flecainide and propranolol. It was suspected that she may have had bouts of SVT at home which may have resulted in her symptoms prior to arrival in the ED.
Debrief Teaching Points – from Thursday Conference
Addendum 11/21/14: To clarify, this patient’s story and exam were more concerning than the frequently encountered ALTE. These points were made by Jennifer and in Jim’s comment (below).
Desiree (Hot Seat Attending) stated it well when she said “This neonate is having worrisome episodes of choking with feeds with projectile vomiting associated with peri-oral cyanosis. This is more worrisome to me than the usual presentation of “ALTEs” with choking but no cyanosis. He is also markedly tachypneic with retractions. I would also like to know if there was any apnea and if the episode of cyanosis self-resolved or if the baby needed stimulation for resolution.”
The case brought up discussions of ALTE and how to not miss a serious diagnosis. Sorry for any confusion.
An apparent life-threatening event (ALTE) is not specific diagnosis but a description of an acute, unexpected episode that is frightening to the caretaker and that includes:
- Apnea
- Color change
- Marked change in muscle tone
- Choking or gagging

The Hot Seat Attending, Desiree, posted a great differential of ALTE: click here to see her comments.
I don’t understand where the discussion about ALTE came from. This is about poor feeding, grunting, and resp distress that has develoiped over a period of 4 days. This is not a lefe-threatening acute event…Jim
Great point Jim & I think Jennifer made a similar comment during Thursday conference.
The term ALTE came up because the mom was concerned with NBNB projectile vomiting that was associated with peri-oral cyanosis. This brought up a brief review and DDX of ALTE. However, this patient had tachypnea, retractions and reports of grunting. The VS & PE were concerning, which prompted an appropriate work-up and eventual admission to the CICU. Great distinction to make!