
Hot Seat #52 Denouement: 21 yo M with painless hematuria
Posted on: March 13, 2015, by : Lenore Jarvis MD MEd
by Astrid Sarvis, Children’s National
with Asha Payne, Children’s National
The Case
The case involves a 21 yo M, presenting with hematuria. This case provides a great reminder of how to approach hematuria in the ED.
Here’s How You Answered Our Questions
At this point, which lab test “would help most” was mixed. All of these tests would help narrow the Ddx, although some are more helpful than others at indicating glomerular vs non-glomerular causes. In terms of imaging, several providers would not order additional imaging or wait, while others would get a CT scan.
Denouement
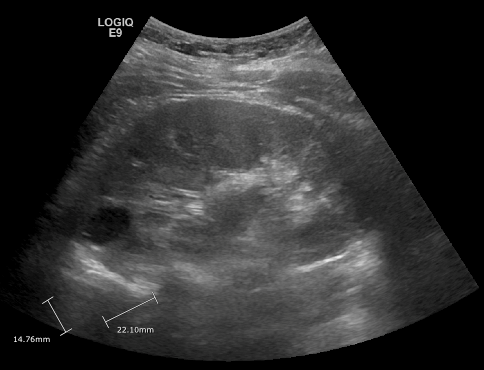
Renal ultrasound read as 7 x 9 mm urachal remnant in addition to 2.4 x 2.2 x 1.8 cm circular structure that represents either a calyceal diverticulum or simple renal cyst.
CT scan with contrast was done in the ED. CT showed urachal diverticulum in addition to a well-defined partially exophytic lesion with renal  mass being on the differential along with renal cysts or calyceal diverticulum.
mass being on the differential along with renal cysts or calyceal diverticulum.
In consultation with nephrology, the decision was made to treat the patient for pyelonephritis. A dose of cefdinir was given in the ED and patient discharged on a 10-day course of ciprofloxacin. Urology was contacted from the ED as well and followup plan arranged.
Urine culture grew Enterobacter aerogenosa (more than 100,000 colony-forming units/mL), susceptible to ciprofloxacin.
The patient followed up with nephrology in 2 days. Labs sent in the ED and during followup including C3,C4, ANA, Adenovirus PCR and Hb electrophoresis all normal.
Teaching Points from Thursday Conference
Hematuria:
After thorough hx & PE, get a UA (w/ microscopic eval), UCx
Most common cause of hematuria presenting to ED is UTI.
Remember to differentiate between hematuria (>5 RBCs) and hemoglobinuria or myoglobinuria (no RBCs w/ positive dipstick).
Causes:

Glomerular: brown or “cola” colored urine, proteinuria (often >2+), dysmorphic RBCs, RBC casts
• Can consider CBC, RFP, C3, C4, ASO, ANA, anti-ds DNA
• If trauma: CT scan abd/pelvis
• Stones suspected: KUB vs ultrasound vs CT
Lower urinary tract: red-pink urine, terminal hematuria, blood clots, minimal proteinuria, normal RBCs
Consider consultation:
Nephrology c/s: HTN, azotemia, proteinuria, concerning FHx for renal failure
Urology c/s: abnormal/concerning GU anatomy, trauma, tumor
Dispo:
Admit: Elevated concern if HTN, edema, oliguria, proteinuria, RBC casts
Discharge: If patient well-appearing without concerning signs/symptoms, especially if microscopic hematuria, outpatient f/u with repeat UA in one week is often appropriate.