
Hot Seat #54 Denouement: 16 yo M w/ back and shoulder pain, now with fever
Posted on: April 9, 2015, by : Lenore Jarvis MD MEd
by Jared Friedman, Inova Children’s Hospital
The Case
The case is an adolescent male presenting with worsening back and shoulder pain x1 week, and fever x3 days, SOB and decr PO intake. The challenge of this case is broadening the differential from a simple sports injury to address his multi-system complaints.
Here’s How You Answered Our Questions
Most physicians stated that they would obtain a chest with/without an abdominal CT (with contrast) to check for abscess, hematoma and intra-abdominal pathology. As the patient is still tachycardic and in pain with limited ROM (in the setting of an unclear etiology) s/p fluid, morphine and anti-pyretics, providers would admit for further work-up and management. Most providers stated that they would likely treat with antibiotics, but felt that more information was needed (e.g. CT scan results) to choose an antibiotic. Others felt that a combination of antibiotics would likely be warranted.
Denouement
CXR read as an ill-defined opacity in the right lung base with small right effusion. Early right lower lobe infiltrate was suspected. An US in the ED showed an unremarkable right upper and lower quadrant examinations; the appendix was not identified. The patient was given ceftriaxone and admitted to the hospitalist service
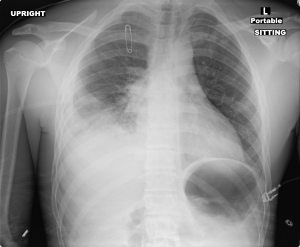
He remained persistently febrile, with right shoulder pain out of proportion (despite PCA pump started), and development of increasing erythema in his neck, pectoral region, and biceps. A follow-up CXR showed increasing lung infiltrates and increasing small right pleural effusion only 30 hours later.
On the Pediatric Floor, due to the above, CT Chest and Neck Soft Tissue was ordered.

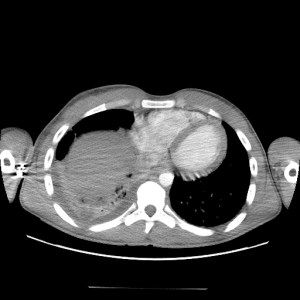

Based on the findings with concern for abscess and his clinical course, concern for a necrotizing soft tissue infection was in the differential. He went emergently to the OR with ENT, Orthopaedic Surgery, and Trauma Surgery, who together made a large incision that tracked from skin, subcutaneous tissues, and clavipectoral fascia finding that the initial abscess seeded through the SCM and deltoid, just stopping short of the right clavicle. Copious chocolate purulent material was evacuated and a wound VAC was placed.
At that point, the patient was then switched from Vancomycin and Clindamycin to Rifampin and Clindamycin per the recommendations of Pediatric Infectious Diseases after the initial wound culture and blood culture grew MSSA. Incidentally, the urine culture also came back positive for MSSA. Finally, the patient slowly recovered and was transitioned to Cefazolin x14 days via PICC and discharged home in 8 days. He was closely followed up, and has now completely returned to baseline.
In summary: Adolescent male w/ MSSA pyomyositis of right shoulder and SCM s/p right SCM I&D, right shoulder/neck/deltoid I&D, and right shoulder washout & closure, MSSA bacteremia/uremia, and MSSA RLL PNA completely resolved 3 weeks out from initial presentation.
Teaching Points
Based on information from UptoDate:
Pyomyositis is a purulent infection of skeletal muscle that arises from hematogenous spread, usually with abscess formation. Predisposing factors include immunodeficiency, trauma, injection drug use, concurrent infection, and malnutrition. 25% to 50% of patients with pyomyositis report a history of trauma with development of infection possibly related to hematoma formation or increased muscle perfusion due to trauma. Staphylococcus aureus is the most common cause and Group A streptococci is the second most common.
Three clinical stages:
●Stage 1 = crampy local muscle pain, swelling, and low-grade fever. Mild leukocytosis and induration of the muscle.
●Stage 2 = 10 to 21 days after onset. Fever, exquisite muscle tenderness, and edema. May have an abscess, and aspiration of the affected muscle typically yields pus. Marked leukocytosis.
●Stage 3 = systemic toxicity. Complications of S. aureus bacteremia (septic shock, endocarditis, septic emboli, pneumonia, pericarditis, septic arthritis, brain abscess, and acute renal failure).
Dx/Tx = Obtain CBC (leukocytosis), ESR/CRP, blood cultures, MRI (preference) or CT (if MRI not available). CK typically normal. Stage 1 pyomyositis can be treated with antibiotics alone. Stage 2 or 3 disease often require both antibiotics and drainage.