
Hot Seat #65: 11yo M with seizure and hematemesis
Posted on: November 12, 2015, by : Jaclyn Kline
Jaclyn Kline MD, Children’s National Health System
Desiree Seeyave MD, Children’s National Health System
The Case
11 year old with epilepsy, last seizure over 2 years ago, presenting after concern for a seizure at home. Per his parents he was watching TV, then got up, was screaming. He then fell to the ground and had 4 minutes of generalized shaking. No rescue medications were given. EMS was called, who did not transport the child. He then started to have bloody emesis, so they drove one hour to your ED. He was vomiting red/brown material en route and also had fast breathing. The parents have a bath towel from the car that has large stains of bright red and brown material on it. They also describe him as being “sleepy” on the way to the ED.
Parents state he has had some recent URI symptoms and is on a course of cefdinir for otitis. They also state that he has ‘big, red tonsils’.
ROS: Positive for vomiting, coughing, seizure as above. Negative for fever
PMH: Epilepsy
Medications: Trileptal
Physical Exam: Vital Signs: T-36.0, HR-145, RR-48, BP- 117/63, O2 Sat-85% on room air
General: Alert. answering questions.
Head: Normocephalic. no visible contusion to scalp, no step offs.
Neck: Supple. no pain with full extension, flexion or lateral rotation.
Eye: Extraocular movements are intact. normal conjunctiva.
Ears, nose, mouth and throat: Oral mucosa moist. large tonsils bilaterally, no visible source of bleeding on exam of tongue and oropharynx.
Cardiovascular: tachycardia, regular rhythm. No murmur. No gallop.
Respiratory: tachypneic with subcostal retractions and nasal flaring, decreased air movement in bases bilaterally, left more than right
Gastrointestinal: Soft. Normal bowel sounds. slightly distended.
Neurological: Alert. face symmetric, tongue midline, able to push against lateral force on face with equal strength bilaterally, able to shrug shoulders bilaterally with equal strength; 5/5 grip strength bilaterally; 5/5 strength with plantarflexion and dorsiflexion bilaterally; finger to nose intact.
You are called to see the child immediately on arrival for hypoxia to 70s, and tachypnea to 50s.
Hypoxia immediately corrects to 98% with placement of non-rebreather, RR in 40s, work of breathing only minimally improves, child is able to speak in short sentences. His hematemesis resolved just prior to arrival.
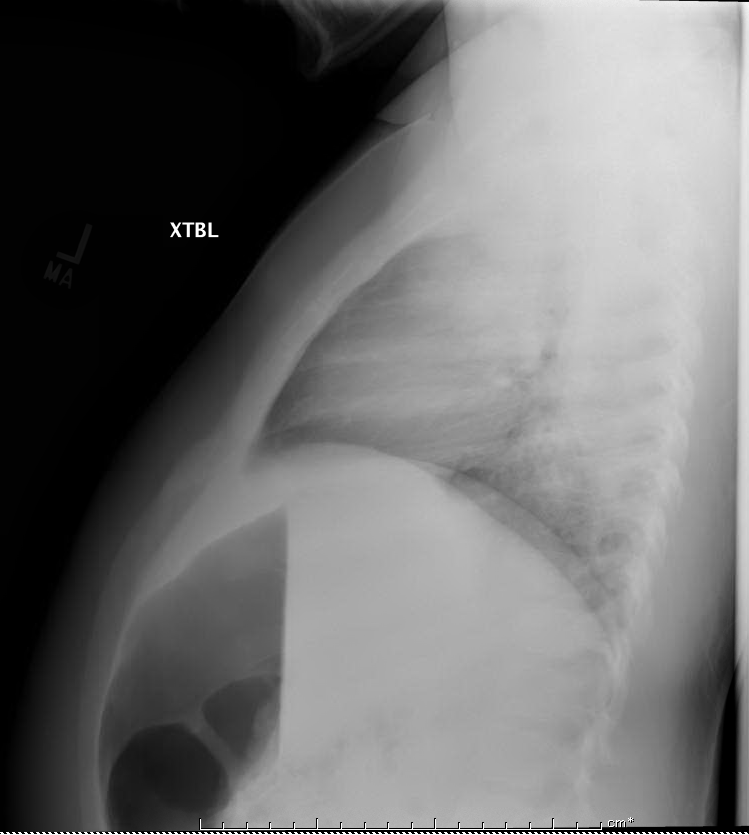
You place an IV and obtain a CBC, coags, and a type and screen (at minimum) with a CXR.
Questions for you:
Update:
WBC-21.3, Hgb-13.9, Hct-40.8, Plt-396, 80% segs, 14% lymphs, 5% monos
INR-1.04, PTT-27.5, PT-13.6
Na-141, K-4.1, Cl-104, CO2-25, BUN-11, C-0.67, Glu-128, Ca-8.8, Mg-2.3, Phos-4.4
Total protein-8.0, Albumin-3.7, ALT-50, AST-55, Alk Phos-556, Total bili-0.2
Guaiac positive emesis

How would you approach this case? Please share your opinions by clicking on “What do you think?” below.
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.
I would definitely put on gloves and a gown and do a quick travel screen for potential contagious things that could require isolation.
it’s always good to try and differentiate hemoptysis from hematemesis. Kids <10yo often can't truly expectorate so he's at the age where this may have been bloody coughing followed by emesis as opposed to coughing followed by bloody emesis…….which helps tell you where it's coming from.
The CXR is concerning for a round lesion in the right lung field which I would suspect is a fungal or bacterial pneumonia and probably needs CT for more information. I think it's easy to suspect an aspiration following a seizure, but it's usually RML and lower lung fields with aspiration…depending on body positioning I guess, so it's conceivable to have upper lobe aspiration if prone from the seizure…but the distribution is a bit odd here.
In any event, the stable hemoglobin, normal coags, normal albumin, and leukocytosis all point to something acute and not chronic.
I wouldn't be thrilled to put him on bipap without normal mental status and the risk for continued pneumonitis. So I would intubate him, send him to chest and head CT, place a PPD, and call the pulmonologists to do a little bronch in the PICU. IF the lungs are clear of blood, it wouldn't be unreasonable to do an upper endoscopy while intubated if able to stabilize his oxygenation. Lots of suctioning for the ETT.
I would bet on a fungal lung lesion that provoked a seizure followed by a blood aspiration event and subsequent hypoxemia/pneumonitis. But I look forward to be completely wrong here and Dewesh solving the crime in just under 3 notes.
Thanks for the intro comments Dave. (With my EMS hat on – I am wondering why EMS did not transport the child — or am I to assume these vitals with resp distress showed up after EMS left?)
Anyway, in thinking of ABC’s – would first consider HFNC to see if it helped more than the non-rebreather. Would have intubation stuff ready to go if no improvement. Would trial this child laying back which would help my decision to intubate – since I want to place him in the scanner to get better imaging of what’s going on with the lungs. If this really is as sudden onset of symptoms as the description portrays, I want a CT because this is NOT how the “run of the mill” pneumonia presents (seizure d/o or not) and I am looking for less common diagnoses to explain this. Is he on something that is resistant to the Cefdinir – like the diff dx that Dave offered above?
GI exam doesn’t comment on abd tenderness — only that there is slight distension. Is pain a component in any of this? I am assuming that lack of pertinent positive findings in the description above means it wasn’t there. So that being said; while the vomiting and blood in emesis is concerning – I am truly focused on airway and breathing primarily. The labs above are reassuring from a GI/Metabolic standpoint so I know I may not “solve” the hematemesis question in the ED – (I am ok with that). But, it needs to be worked up and my perspective is to determine whether it is related to the concerning respiratory issues the patient is having or whether it is a separate process.
So ultimately, I focus on getting this patient out of the respiratory danger zone as best I can – NRB improved things a bit; so I then see if I can get a little further ahead with a HFNC. If that works, I know I am admitting to PICU. He gets fluids and IV abx in ED. If he needs to be intubated to tolerate CT or because he continues to decompensate, then I do that in the ED. Otherwise, I think the rest of this is inpt work up – they can do GI lavage, bronch etc up there and depending on the chest CT results start focused treatment.
11 yo M with seizure and hematemesis.
Like Dave stated, it can be difficult to differentiate between blood from the GI tract and the lower and upper respiratory tract or nasopharynx in kids.
Let’s talk about hematemesis first. The differential includes:
– Gastric and duodenal ulcers
– Gastritis
– Esophagitis
– Esophageal varices
– Blood vessel disorders e.g. Ehlers-Danlos, hereditary hemorrhagic telangiectasia (can also cause hemoptysis)
– Bleeding disorders
– Liver disease
– Mallory-Weiss tears
I would ask about a history of abdominal or chest pain, reflux, NSAID use, family history of bleeding disorder, bleeding from other places, feel for hepatosplenomegaly. The normal LFTs and coagulation studies are reassuring that liver disease is unlikely.
From here, I would move on to bleeding from the respiratory tract. Also, given the CXR findings and the large RUL and LUL consolidations, I would hone in more on the lower respiratory tract as the source of bleeding. (It’s mentioned that his tonsils are large but not obviously the source of bleeding)
Hemoptysis:
– Pneumonia – TB, bacterial, aspiration
– CF
– Bronchiectasis
– SLE
– FB aspiration
– Trauma
Further history needed would be h/o cough/congestion, fever, sick contacts, travel, exposure to TB, family history of genetic disorders or autoimmune diseases.
How does this tie in to having a seizure disorder? Did he have a seizure and then aspirate? The timeline seems to be almost too immediate for development of hemoptysis/hematemesis after the seizure. Did he have a pulmonary process/infection that lowered his seizure threshold? This seems more likely.
The respiratory distress, hypoxia that responds to O2 by NRB, high wbc count with left shift supports the diagnosis of bacterial pneumonia.
I can’t help but think about his seizure disorder. Did he ever have brain imaging? Could he have hereditary hemorrhagic telangiectasia causing brain AVMs and hence seizures, and now pulmonary hemorrhages?
Also, rare but serious side effects of trileptal include abnormal liver enzymes, thrombocytopenia and bleeding, usually from the nose or gums, but bleeding can occur anywhere.
I wait with bated breath for the big reveal…