
Hot Seat #70 Denouement: 14 yo F w/ continued low-grade fever and cough
Posted on: March 10, 2016, by : Lenore Jarvis MD MEd
Jared Friedman MD, INOVA Children’s Hospital
with Jennifer Chapman MD, Children’s National Health System
The Case
14 yo F history of mild intermittent asthma with multiple bouncebacks to the PMD and Peds ED due to continued, worsening fever and cough. The challenge of this case was how to best address diagnosis/treatment at each step in her progressive illness.
Here’s How You Answered Our Questions
Other:
Q1: Look at lateral chest X-ray and review with radiologist. ? Complicated pneumonia
Q2: treat sepsis
Denouement
She had failed outpatient treatment and was therefore admitted to the Peds Hospitalist for further evaluation and management after she received NS bolus x2, Tylenol x1, Ceftriaxone x1, and Vancomycin x1 in the ED.
The patient was continued on Ceftriaxone and Vancomycin (until blood cultures were negative x48 hours). Pediatric Infectious Disease and Pulmonology later recommended to continue on Ceftriaxone, add Azithromycin (RVP came back RSV+), and change the Vancomycin to Clindamycin, as well as pulmonary toilet, incentive spirometry, and Albuterol PRN.
However, the patient continued to be persistently febrile and a follow-up CXR and U/S showed continued presence of the consolidation and effusion. Pediatric Surgery was consulted for possible VATS procedure. Yet, due to the fact that she never required supplemental oxygen and was not in respiratory distress, this invasive procedure was not recommended.
Atypical laboratory tests (see below) were sent off, and the patient was then switched from Clindamycin to Doxycycline for possible resistant mycoplasma or other atypical pathogens. After an additional 48 hours (4 days total in the hospital), the patient defervesced and was switched to Cefdinir two days prior to discharge home.
In summary: 14 year old female with PMH of mild intermittent asthma, presenting with LUL PNA with parapneumonic effusion in the setting of an acute RSV+ and strep pharyngitis infection requiring admission after failed outpatient therapy.
Atypical laboratory tests normal: Psittacosis, Q-fever, Fungal antibody panel, TB – Quantiferon gold, Mycoplasma pneumoniae, Legionella pneumophilia, Histoplasma urine ag
However, her parents requested a full immunoglobulin work-up with concern about common variable immunodeficiency.
Follow-up CRP: 0.9
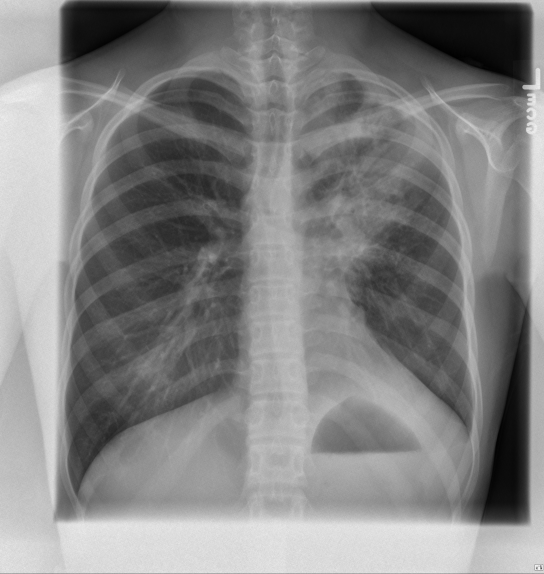
Follow-up CXR:
Teaching Points
Radiologists are our friends!
Look at the lateral XR. When confused/concerned about an image, don’t be afraid to call the radiologist to ask about what is going on. They can also help to guide additional imaging modalities.
The indications for pleural ultrasound include: detection of pleural fluid or a pneumothorax, guidance for diagnostic and therapeutic thoracentesis, and guidance for placement of thoracostomy tubes.
CT provides a more detailed view of the internal organs and structures than CXR or ultrasound.
 .
.