
Hot Seat #84: 3yo F w/ Hip Pain
Posted on: November 7, 2016, by : scott herskovitz
Scott Herskovitz MD, Inova Children’s Hospital
with Shireen Atabaki MD, Children’s National Medical Center
The Case
A 3yo female presents to the ED with right hip pain for the past 2 weeks. Her mother states that the patient was lying prone on a swing set going back and forth when she “jammed her leg into the ground.” She has been limping and complaining of pain since the event.
ROS: No rash, no fevers, no weight loss, no night sweats, no chills
PE:
VS: T 37.2°C BP 102/68 HR 125 RR 28 S 100% Ht 0.965m Wt 15.3 kg
GENERAL: In no apparent distress. Awake & alert. Not diaphoretic.
HEENT: Atraumatic, Normocephalic, Mucous membranes are moist and intact. Posterior pharynx is clear, no exudates. External inspection of the ears reveals no abnormality. No appreciable lymphadenopathy. Neck is supple.
CARDIOVASCULAR: Regular rate and rhythm, no murmurs, rubs, or gallops. Peripheral pulses are 2+ and equal.
PULMONARY/CHEST: Clear to auscultation bilaterally
ABDOMINAL: Soft and non-distended. No tenderness.
MUSCULOSKELETAL: Right hip tenderness with palpation, complains of pain at the hip when ranged. no swelling, no erythema, normal exam to ipsilateral knee, ankle, foot, and contralateral leg. Antalgic gait.
SKIN: Skin is warm and dry. No diaphoresis, rashes, or lesions.
NEUROLOGICAL: Alert, awake, and appropriately oriented.
Question:
Xrays are obtained:


After motrin, her gait is normal and her pain and tenderness resolve. She is discharged home with orthopedic follow up.
The patient returns to the emergency department two days later with the chief complaint of abdominal pain and fever. The abdominal pain started in the morning, was nonspecific, non-radiating, and associated with a few episodes of vomiting and diarrhea. The parents also endorse myalgias and arthralgias that they think are localized to the lower extremities. Temperature at home today was 102F. The patient attends preschool and has not had any recent travel. She is up to date on all vaccines and has been otherwise healthy. There are no rashes.
PE:
VS: T 38.9°C HR 150 BP 120/65 RR 26 S 97% RA
GENERAL: Alert, well-appearing, comfortable in bed sitting upright, NAD
HEENT: PERRLA MMM. PO w/o exudate/petechiae/ulcers/blisters
PULMONARY/CHEST: CTA b/l – no wheezes/crackles/flaring/retractions.
CARDIOVASCULAR: Tachycardia with regular rhythm. nml s1,s2 no m/g/r. WWP, CR<2 sec, +2 pulses b/l
ABDOMINAL: Soft abdomen, ND. No HSM appreciated. No flank/CVA/back tenderness.
SKIN: No rash on body.
MUSCULOSKELETAL: Moves all extremities b/l except at the hips. R>L hip pain with ROM and TTP. No obvious erythema or swelling at the joint. Ambulates with antalgic gait favoring R leg.
Question:
Results:
WBC 6.6 H/H 8/25 Plt 235
Na 137 K 4 Cl 105 CO2 18 Ca 9.5 BUN 11 Cr 0.6 Glucose 151
CRP 29
ESR 106
Flu negative
An ultrasound of the hips reveals the following:
Right: 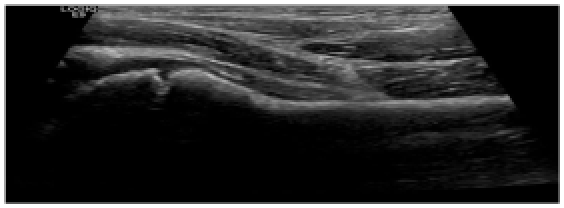
Left: 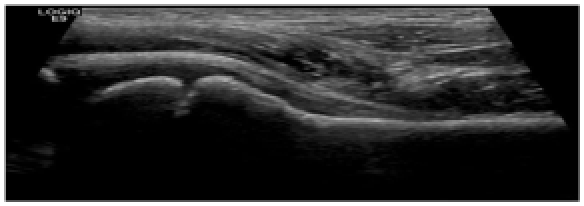
Question:
How would you approach this case? Please share your opinions by clicking on “What do you think?” below.
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.
I don’t think the US adds anything here. The first clinical decision you need to make is whether this is a septic joint that requires debridement in the OR. Neither The history nor exam is suggestive of this but absolutely points to an inflammatory source. Even with an effusion on US, this does not exclude the possibility of a concomitant osteomyelitis, especially of the proximal femur or acetabular area. Osteo classically arises after a minor trauma that seeds a metaphysis. Without the trauma I would probably be more thorough to exclude something spine or neurologic. If you work in an IR aggressive hospital, an US guided joint aspiration is not unreasonable if there is a sizable effusion without a classic septic joint presentation. But our local institutions favor MRI as next diagnostic choice. Since this child has abdominal pain, a perforated appendicitis or psoas abscess is also a possibility.
The bigger question is why is the kid’s Hb=8 ? This argues for a chronic disease. This may make a malignancy higher on the list so I might be a bit more thorough and add something like a CXR, albumin, retic count and LDH. Someone teach me why we did an ultrasound here. Especially with full ROM of hip? I’d probably get a little more information before putting the kid through a sedated MRI. Don’t want to find something that requires a second sedated exam.
I’m going to politely disagree with Dave about the utility of an ultrasound. If she had normal labs I might skip it. However, a negative XR study + inflammatory markers means we have to investigate a little bit more. Especially with the anemia: we still need to see a differential even if the WBC appears within normal limits. We also see enough Lyme in Northern VA that lyme arthritis is not ruled out for me (and won’t be ruled out tonight either), but agree that we need more information.
An ultrasound is easy to do and is not harmful. I know, I know, if it’s negative, you still have to keep looking. But it’s not going to need a stat washout and gives you a chance to look elsewhere and wait for those other studies to come back. Agree with other tests, especially LDH. A spine film might also be helpful if there is antalgic gait. (By the way fellows, think about how you might have to manage this if you’re not at a tertiary peds center? What if the patient is coming from an hour away from a pediatrician’s office with these labs already done? if they don’t have a PMD?) This case would be a punt. IR is not going to be tapping a 3 yo hip, they’re going to punt to Ortho, who are going to punt it to Peds Ortho, in which case they’ll be transferred to you.
From my experience, if at this point you consult Ortho, they will probably ask for an ultrasound. If you skip this and ask for an MRI, the radiologist will most likely ask for an ultrasound. At our place we couldn’t possibly get a sedated MRI in the middle of the night. We also have to manage expectations.
So in this case just do it.
DDX: occult fracture, myositis, pyomyositis, osteomyelitis, or other bony process…Heck, throw in lead poisoning too. Walled off abdominal psoas abscess…would expect fever by now, but we’ve seen plenty without.
I would suggest a conservative approach, and concur with the initial us to assess for effusion, and would suggest a sedated MRI of the hips at this point. The child should be kept npo and a blood culture also obtained. The child is febrile (T 38.9) with an elevated esr and crp and a septic joint or osteomyelitis need to be ruled out, even though the patient does not have evidence of leukocytosis.
The presentation is fairly acute, especially with the preceding trauma potentially seeding an infectious etiology.
Yes an evaluation for Lyme arthritis is possible but the acuity and temp of 38.9 and preceding trauma make that less likely and would be considered in the secondary evaluation. I would not image the spine at this stage due to the bilateral hip pain and suspicion for infectious etiology, unless the patient had focal tenderness over the spine (which is not the case here) and discitis would then be in the differential. The same is true for an intra-abdominal abscess or appendicitis as the belly is non tender.
The work up for malignancy would also be in the secondary evaluation if nothing else showed up in the initial evaluation. I agree the Hb of 8 is concerning but in a 3 yo there is a possibility that this could be due to the child still primarily consuming cow’s milk and iron deficiency anemia is in the differential and a thorough dietary history, MCV and Ferritin can help determine the etiology.