
Hot Seat Case # 99: 14 yo F with abdominal pain
Posted on: September 23, 2017, by : scott herskovitz
Scott Herskowitz, MD Inova Children’s Hospital
with Emily Willner, MD Children’s National Medical Center
A 14-year-old female presents at 0100 with acute on chronic abdominal pain with weight loss and new onset vomiting. She has had vomiting once a day over the past 3 days that has been nonbloody and nonbilious with poor oral intake and epigastric pain for the past 2-3 months. Her pain is worsened with oral intake and currently 5/10. Over this time she has been diagnosed with GERD and started initially on Pepcid without improvement and she is currently on Zantac. She was seen in an outside emergency department 1 week ago due to abdominal pain with normal CBC, CMP, lipase and no imaging performed. Denies recent travel.
ROS: No rash, no fevers, no night sweats, no chills, no syncope, no palpitations
FHx: maternal aunt w/ thyroid disease
Meds: Zantac
Exam: T 98.4 °F BP 107/72 HR 87 RR 18 O2sat 98% Ht 162.6 cm Wt 49.5 kg
General: Alert, well-appearing, comfortable in bed sitting upright, NAD talking to Mom in bed
HEENT: PERRLA/EOMI, MMM PO w/o exudate/petechiae/ulcers/blisters, no appreciable lymphadenopathy or thyromegaly
CV: RRR nml s1, s2 no m/g/r, WWP, CR<2 sec, +2 pulses b/l
Pulm: CTA b/l – no wheezes/crackles/flaring/retractions
Abd: Soft abdomen, ND. No HSM appreciated. No flank/CVA/back tenderness.
Mild tenderness in epigastric area. No RLQ point tenderness. No rebound or guarding. No Rovsing sign
MSK: Moves all extremities b/l, no deformity
SKIN: Moist. No rash, no pallor, Gray color
NEUROLOGICAL: Alert, awake, and appropriately oriented.
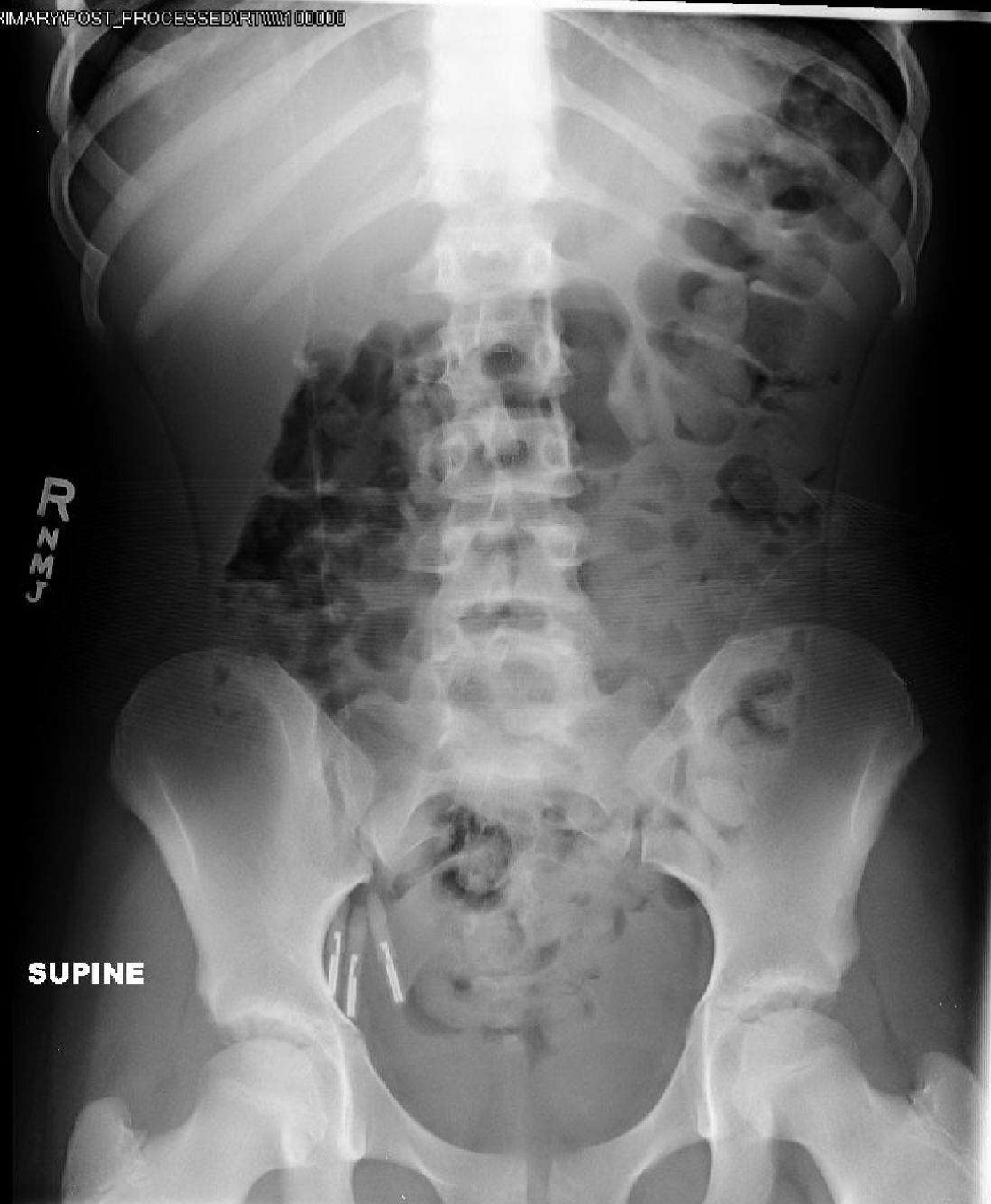
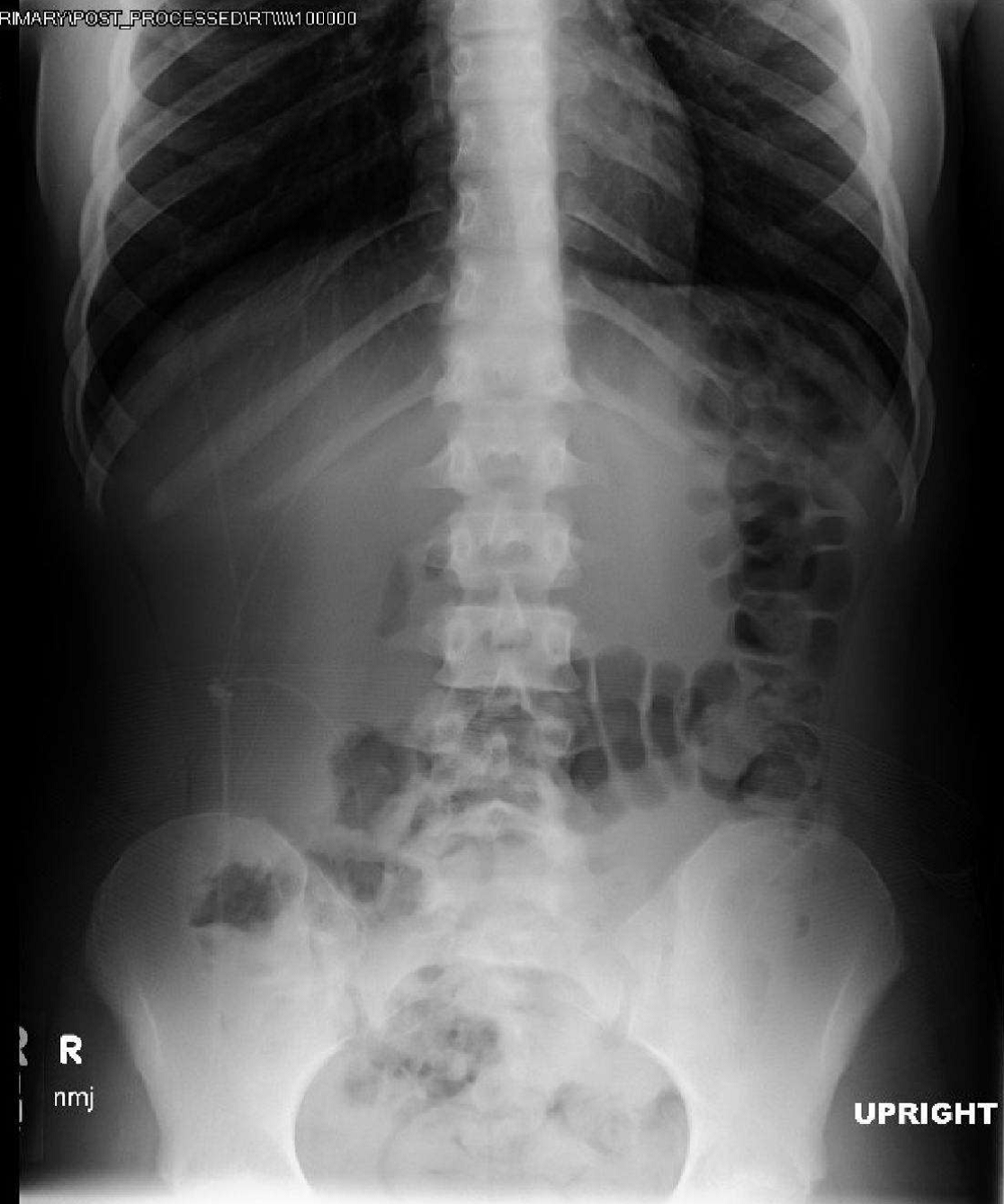
Xray of the abdomen is obtained:
After motrin, fluid bolus, protonix and zofran her pain is minimally improved but she has no vomiting and is tolerating PO.
The following labs have resulted and repeat v/s:
WBC 7 H/H 15/40 Plt 211
Na 127 K 5.5 Cl 97 CO2 20 BUN 15 Cr 1.2
Liver enzymes, Lipase, CRP, ESR all unremarkable
Pulse 68 | BP 93/56 mmHg | Resp 20 | SpO2 99 % |
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.
So essentially, we have an adolescent female with nonspecific, intermittent abdominal pain, gray skin (I like how that was snuck in there!) and hyponatremia. Anybody work up porphyria yet? The differential also includes heavy metal intoxication such as argyria (chronic silver intoxication) and arsenic.
I think when someone hands you hyponatremia….it’s one of the times we can feel smart as ED docs by honing in on a diagnosis. It doesn’t take an ER doc to send a CBC and CMP. think about SIADH? salt-wasting? renal? exogenous? drugs? cortisol?
catch some pee and calculate a fractional excretion of Na.
=NaU*CrP / NaP*CrU
this at the least helps distinguish pre-renal from renal disease.
I don’t know what grey skin is on someone who is outside the code bay, but tan (hyper-pigmented skin in Addison’s disease) would make sense here……..low Na, high K………..:)
Differential is huge here so try a stepwise approach starting with FeNa so you’re not racking up a crazy bill with unnecessary tests!