IOTW: Dilated Cardiomyopathy
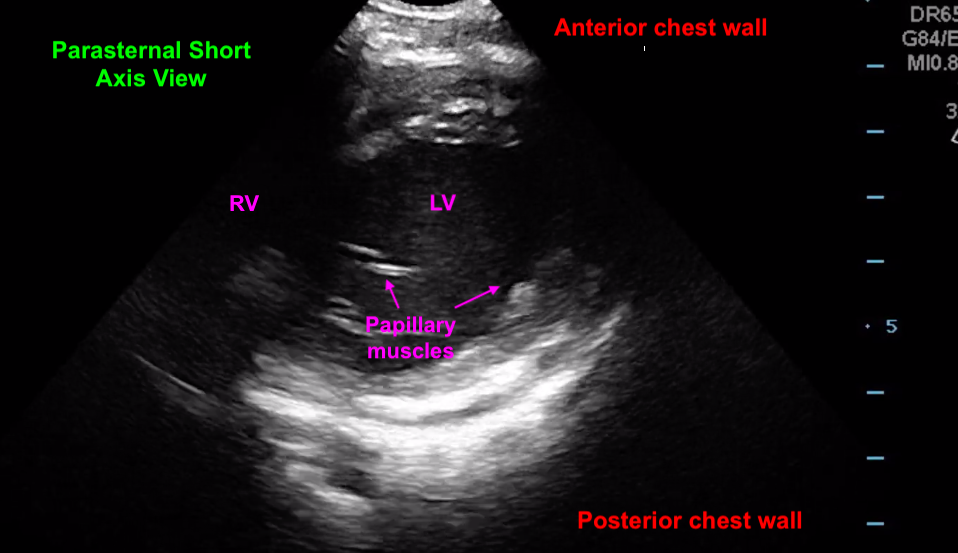
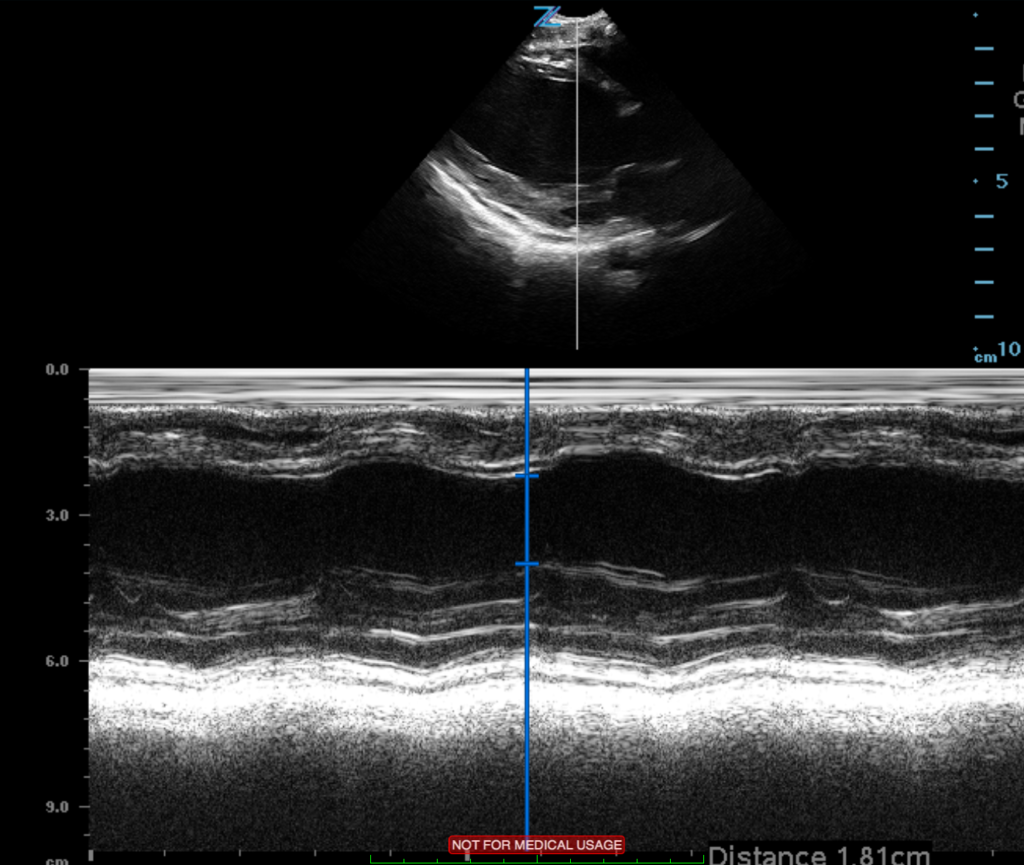
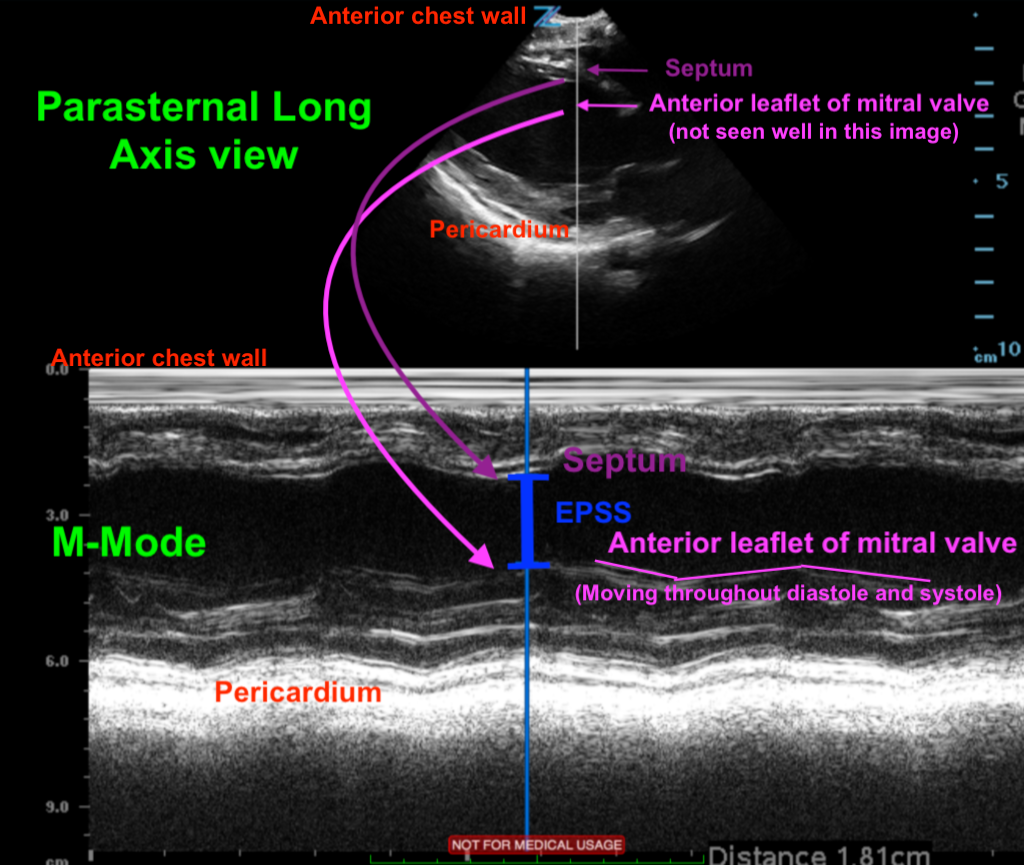
Posted on: January 23, 2020, by : Mary Kate ClaiborneThis patient is a 9yo F with PMH of dilated cardiomypathy who presented to the UMC ED for fever and tachycardia with a family member who was influenza A+. Cardiac POCUS was performed. Patient was noted to have enlarged left ventricle with grossly decreased function. Left ventricular ejection fraction (LVEF) was estimated using E-point septal separation (EPSS). EPSS is obtained in the parasternal long access view using M-mode which shows motion of the ultrasound wave over time. M-mode can be used to trace the movement of the mitral valve to calculate the EPSS. During diastole, the ventricle fills with blood and the anterior leaflet of the mitral valve swings open toward the interventricular septum. When the mitral valve leaflet reaches its maximal excursion and is closest to the septum, the distance between the two can be measured and is called the EPSS. A normal EPSS is <7mm. This patient’s EPSS was 18.1mm, indicating decreased left ventricular ejection fracture. Cardiac POCUS was compared to prior ECHO by cardiology fellow and was found to be this patient’s baseline function, so patient was able to be discharged home without transfer to CNMC.