
Ultrasound Evaluation of Not Your Average Dyspnea
Posted on: February 18, 2018, by : Haroon Shaukat MD
Case:
A 14 year old female with history of a mediastinal tumor resection presents with worsening chest pain for one week. She complains of dyspnea and sharp mid-sternal chest pain. She is currently undergoing chemotherapy and radiation treatment. On the day of presentation, the patient had a syncopal episode with a prodrome of “floaters and spots”. She denies recent fevers, recent illnesses, or poor oral intake.
She was initially evaluated at an outside hospital where she was found to be hypotensive and required 2 fluid boluses for resuscitation. She was treated presumptively with antibiotics. Her labs were significant for a WBC 19k with 88 PMN’s and normal platelets. Her chest radiograph was normal.
Physical Exam:
T 36.8 HR 131 RR 40 BP 100/72 SpO2 100% on RA
The patient is alert and cognitively intact with moderate respiratory distress. She has normal capillary refill, but is tachycardic without a murmur or gallop. Her lungs are clear bilaterally but tachypneic with intercostal and subcostal retractions. Her abdomen is soft and non-distended without tenderness to palpation or organomegaly. She has no focal neurologic deficits.
Point-of-care ultrasound (POCUS) findings: Cardiac
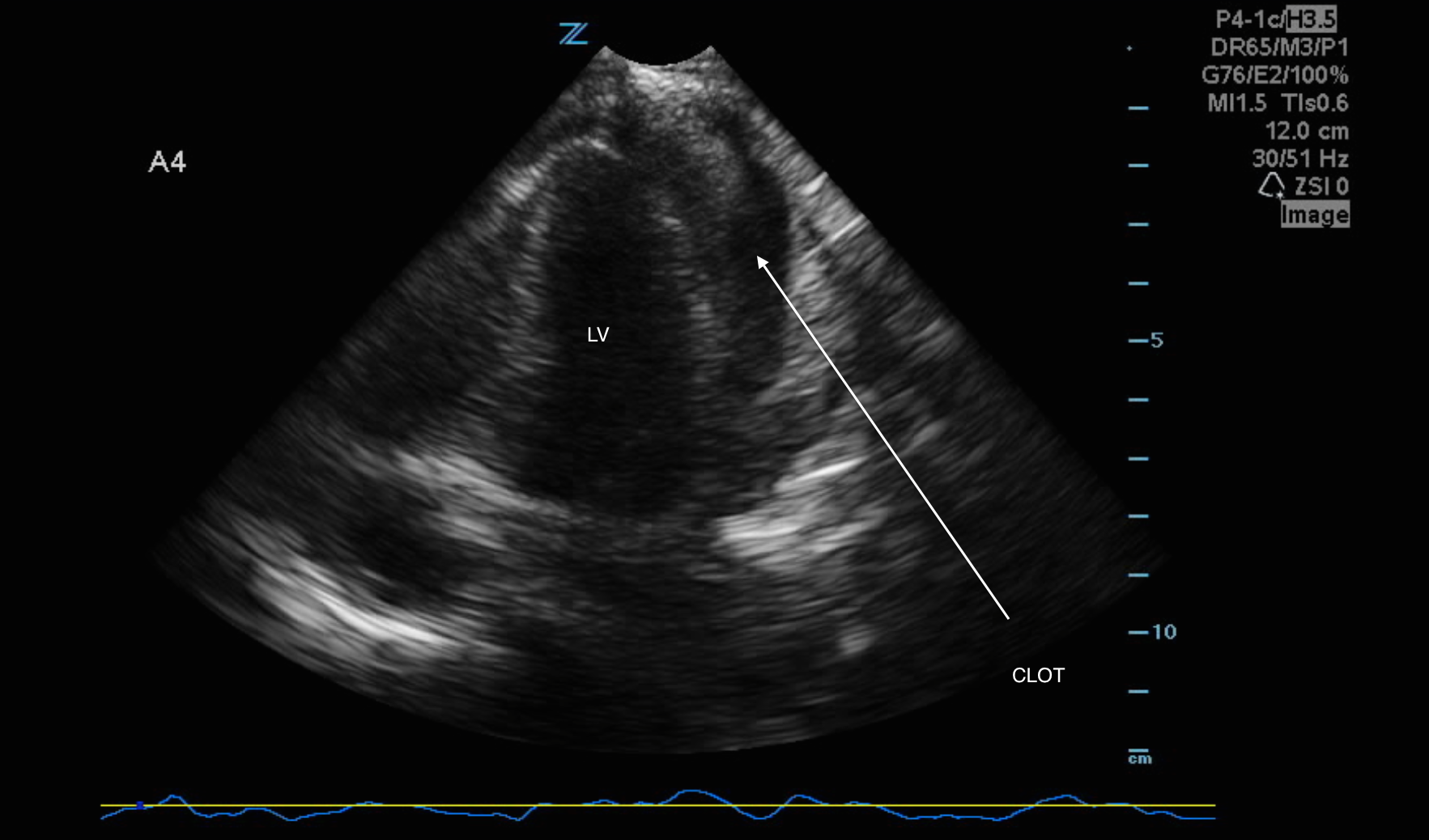
Bedside Interpretation: Apical four chamber view showing a large pericardial effusion posterior to the left ventricle.
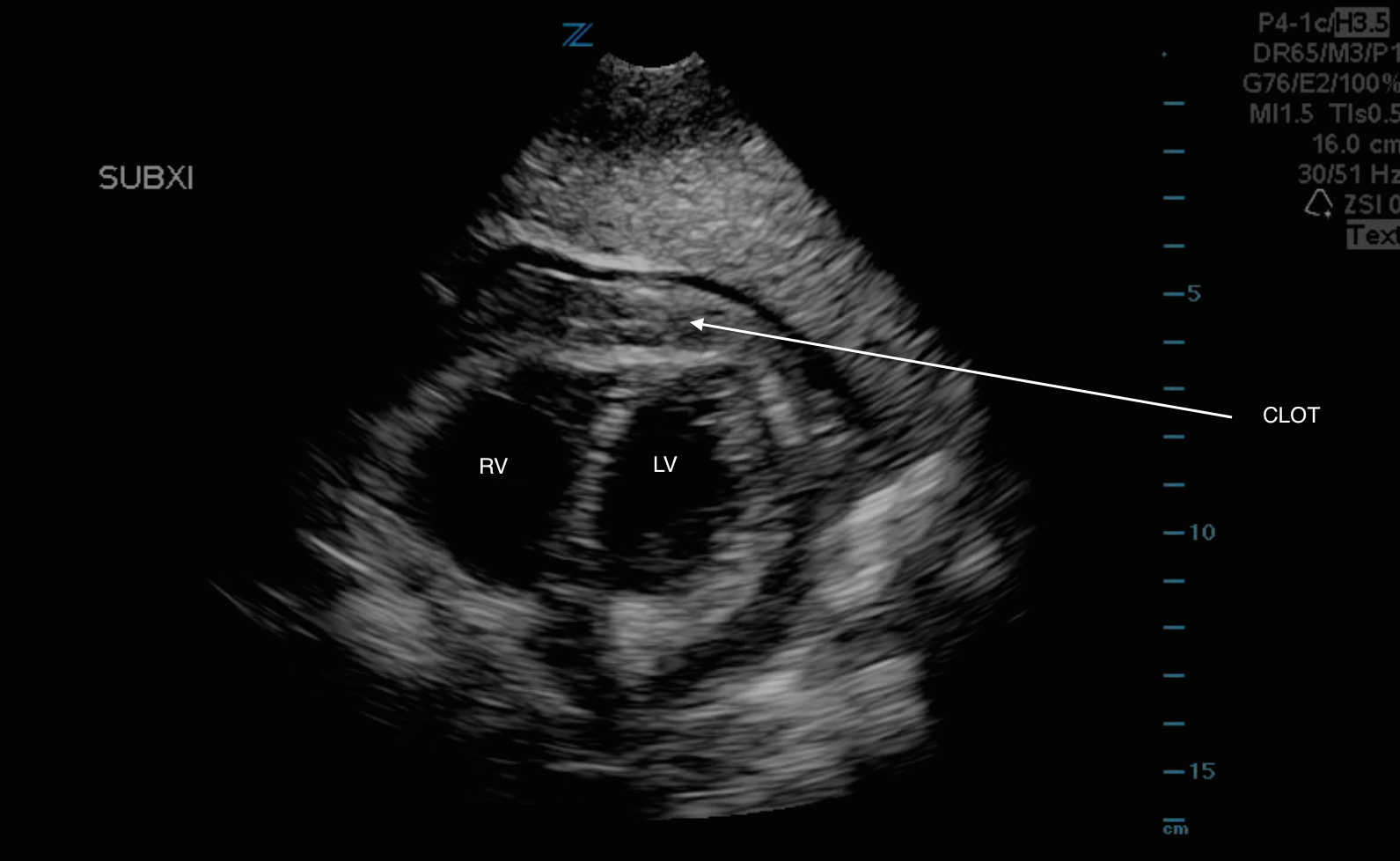
Bedside Interpretation: Subxiphoid view showing the pericardial effusion with a large echogenic collection eluding to a complex fluid collection, presumably a blood clot.
Bedside Interpretation: Subxiphoid view again showing the pericardial effusion with echogenic material, however, the function of the heart is maintained.
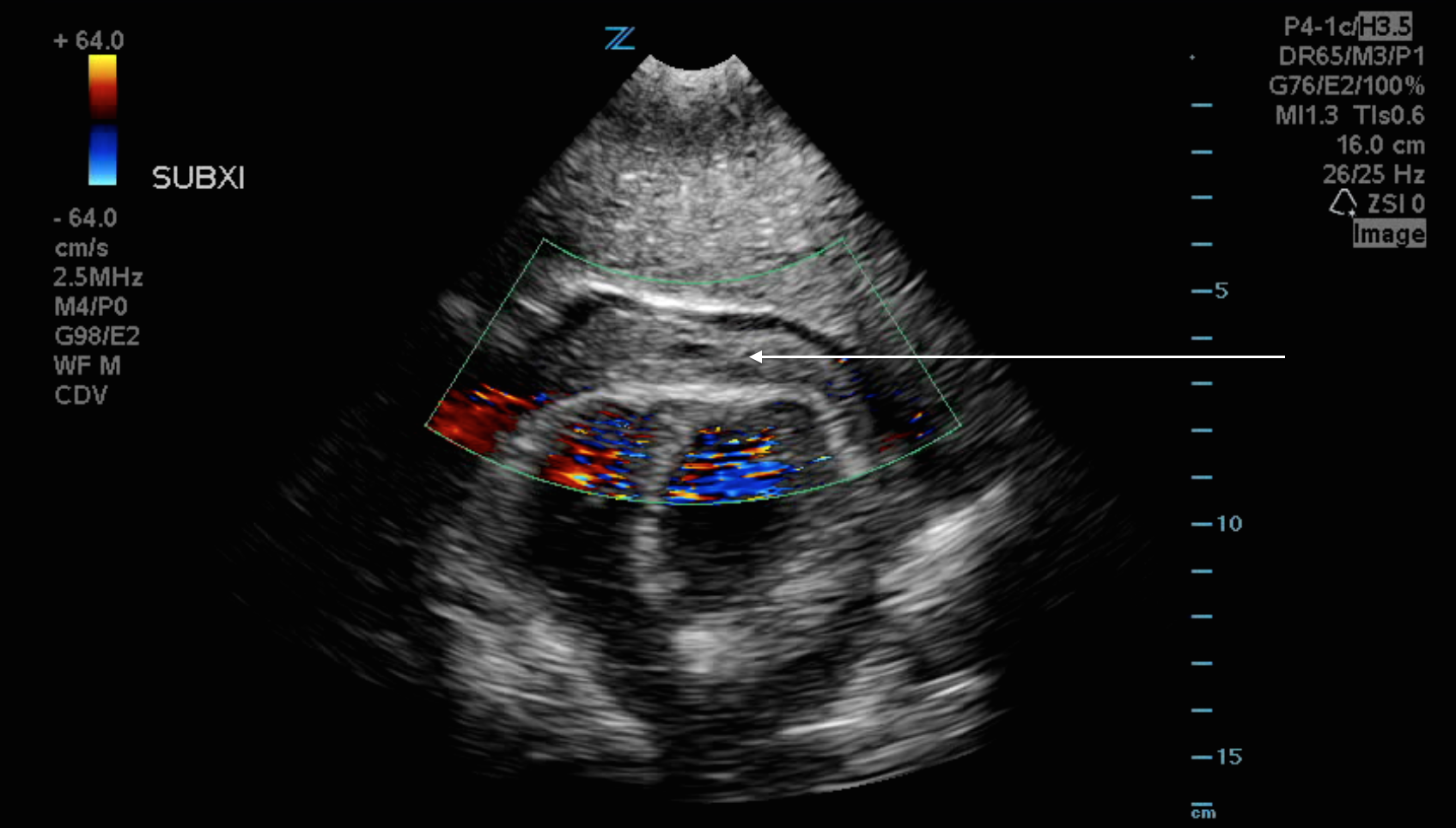
Bedside Interpretation: Similar to the previous image, however, with overlying color flow.
ED Course:
The patient was noted to be hemodynamically stable and her pain was controlled. antibiotics were broadened and a Computed Tomography Angiography of the Chest was obtained to ensure there was no concomitant pulmonary embolus, of which there was not. It did, however, confirm a large (1.8 cm) pericardial effusion with an associated pleural effusion.
Cardiology was consulted and the patient did not have evidence of tamponade on echocardiogram, however, did progressively have worsening tachypnea, tachycardia, and chest pain. She remained on room air but given her worsening status, she was admitted to the CICU and a pericardial drain was placed removing several hundred cc’s of sanguineous fluid.
Discussion:
Any pericardial disorder can essentially produce a pericardial effusion, although a majority will result from: acute pericarditis, autoimmune diseases, cardiac surgery, sharp/blunt trauma to the chest, malignancy, or mediastinal radiation [1]. Unless cardiac tamponade is present, physical exam findings are extremely nonspecific; in fact, most patients’ symptomatology will be related to the underlying disease process [2].
Echocardiography is usually required to establish the diagnosis of a pericardial effusion, although other studies are often helpful including a chest radiograph and electrocardiograph. Echocardiography is not only specific and sensitive for the detection of pericardial effusions, but also can give information regarding its effect on hemodynamics. Small collections (25 to 50 cc’s) are often physiologic and typically seen posterior to the left ventricle. However, fluid above the right atrium in the apical four chamber view is often argued as the single most specific and sensitive indication of a pericardial effusion [3].
A pitfall to cardiac ultrasound is that pericardial effusions are not always easy to visualize. They are usually anechoic, however, that may not be the case in a complex collection that could include clots, pus, or fibrin. Pericardial effusions can be circumferential or regional, but even when circumferential, fluid may distribute irregularly. According to Blanco and Volpicelli, the most important tips involving pericardial effusions are to: 1) track anterior to the descending aorta in the PSL and apical four views. 2) They will always present in dependent segments (posterior, lateral, and inferior walls). 3) Check the diastolic collapse of cardiac chambers as it can be a sign of a hemodynamically significant effusion. [4][5][6]
[1] Levy PY, Corey R, Berger P, et al. “Etiologic diagnosis of 204 pericardial effusions.” Medicine. 2003. 82: 385.
[2] Hoit BD. “Diagnosis and treatment of pericardial effusion.” UpToDate. https://www.uptodate.com/contents/diagnosis-and-treatment-of-pericardial-effusion. Accessed January 30, 2018
[3] Adler Y, Charron P, et al. “2015 ESC Guidelines for the diagnosis and management of pericardial diseases.” Eur Heart J. 2015; 36: 2921.
[4] Blanco P and Volpicelli G. “Common pitfalls in point-of-care ultrasound: a practical guide for emergency and critical care physicians.” Crit Ultrasound J. 2016; 8: 15.
[5] Strony R, Linkenheil E. How to delineate pericardial effusion from pleural effusion on bedside ultrasound. J Emerg Med. 2016;50(3):495–496.
[6] Goodman A, Perera P, Mailhot T, Mandavia D. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade. J Emerg Trauma Shock. 2012;5(1):72–75.
The information in these cases has been changed to protect patient identity and confidentiality. The images are only provided for educational purposes and members agree not to download them, share them, or otherwise use them for any other purpose.
Interesting case!