
Hot Seat #180: A 13 yo with Leg Pain
Posted on: November 23, 2021, by : Walter Palmer
By Chris Kovaleski, Inova LJ Murphy Children’s Hospital
A 13-year-old boy with history of mild Factor IX deficiency presents to your ER with leg pain following a bicycle accident approximately 20 minutes prior to arrival. He states that he was riding his bicycle, un-helmeted and fell after hitting a bump in the road. He is now complaining of right hip pain. Reports no loss of consciousness, pre-syncopal symptoms or witness-reported seizure activity. Has never had hemarthrosis or required factor before. Up to date on immunizations.
ROS: Denies headache, nausea, vomiting, numbness, tingling, bleeding, bruising
Exam: VS Afebrile, HR 73, RR 20 BP 112/74, 100% on RA
Primary Survey intact
Head/Chest/Back/Abdomen with no signs of trauma, TTP
No pelvic instability
Neck with no bony tenderness and full ROM
Scattered abrasions to anterolateral R thigh, exquisite TTP to R hip and femur. Neurovascularly intact in affected extremity with good capillary refill, no focal numbness/tingling, evidence of hemarthrosis. Minimal swelling noted to area of injury. ROM exam limited by pain.
Imaging:
FAST negative
Reassessment following meds notable for improved pain, no significant change in vitals/exam. CBC with CBC of 9.1, Hgb of 14.5/HCT of 42.6, Platelets of 290. Coags WNL. CMP with glucose of 140, BUN of 19, Cr 0.9, electrolytes and LFT’s WNL.
X-rays of affected hip/pelvis, femur and tib-fib are obtained are notable for no detectable fracture or focal lesion and soft tissues are unremarkable. Approximately 1.5 hours following arrival in the ED, vitals and exam are unchanged and pain is controlled following initial fentanyl administration. Specifically, there is no evidence of hemarthrosis, change in leg swelling, change in neurovascular status or mental status.
Decision made to discharge home with plan to follow up with PMD as needed. However, the patient reports significant pain with ambulation and is unable to bear weight on affected extremity, even with use of crutches.
Ultrasound of the right thigh was performed which revealed the following:
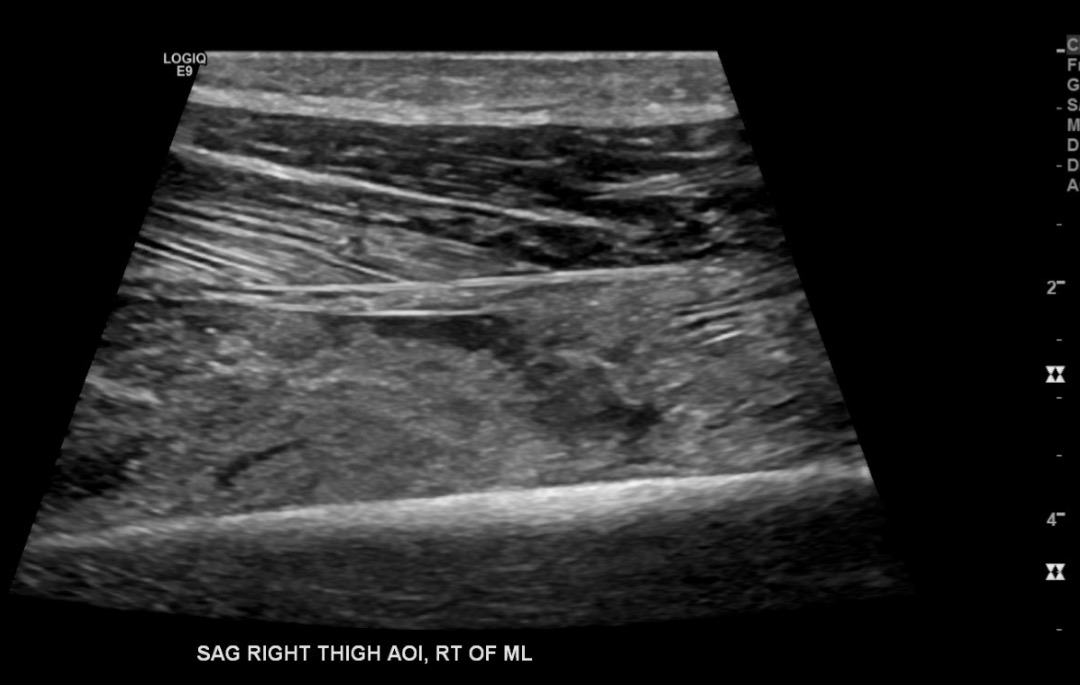
Ultrasound notable for a 4 cm laceration defect involving the vastus intermedius muscle with associated small hematoma and hypoechoic tract that includes blood and surrounding soft tissue edema. Discussed with orthopedic surgery with concern for Morel-Lavallee lesion (closed degloving injury with separation of dermis from fascia) vs isolated muscle laceration.
I think it would be good to clarify the “history of mild Factor IX deficiency” — i.e., how was this diagnosis made, what is his usual factor level, what is the treatment plan for severe injuries, etc.? The fact that his coags are WNL is reassuring and argues against emergent need for factor transfusion before first speaking to Hematology.