
Hot Seat #54: 16 yo M w/ back and shoulder pain, now with fever
Posted on: April 1, 2015, by : Jared Friedman
by Jared Friedman, Inova Children’s Hospital
The Case
16 year old p/w back and shoulder pain x1 week, and fever x3 days. Seen at an OSH 6 days prior to visit with right shoulder pain after playing basketball. XR then was negative, was given Motrin, and sent home. However, he has had worsening right shoulder pain spreading to the right RUQ and right lower back pain causing him to “walk with a hump.” Fever (TMax 102F PO) started three days prior to this ER presentation, was relieved with Motrin and/or Tylenol (last given night prior to visit). He also complains of shortness of breath and difficulty breathing worse at night, needing to sit upright in bed. No cough. +decreased PO x2 days (but tolerating liquids), and has a sick contact at home with URI symptoms.
ROS: No vomiting, diarrhea, lower abdominal pain, headache, photophobia, dysuria, trauma, changes in mental/neurological status, rash.
PMH: Clavicle fracture 2 years ago
Physical Exam: VS @ Triage: BP130/71 HR102 T104.6 RR20 O2 98% Height/Weight: 65%
Constitutional: Alert, non-toxic, but uncomfortable and in pain complaining of right shoulder/back/upper abdomen pain sitting at 80 degrees in bed.
HEENT: PERRLA/EOM, MMM, TM’s normal w/ light reflex b/l. Clear OP.
Neck: Supple, normal ROM on extension/flexion/rotation. No LAD. Mild redness around site of hot pack over R lower neck/clavicle/shoulder. No crepitus.
Chest/Respiratory: Mild decreased breath sounds right lung base, but splinting/not deep breathing. No wheeze/crackles. No tachypnea or retractions/flaring
CVS: tachycardic, RRR, no murmur, +2 pulses x4.
Abdomen/GU: +BS, soft, ND, no HSM appreciated. RUQ tenderness, +Murphy’s sign. +Right CVA pain w percussion.
Musculoskeletal: FROM x3 when sitting up at 80 degree angle in bed. decrease full extension/flexion/rotation of right arm secondary to pain. Not focally TTP.
Skin: WWP, CR less than 2 sec throughout. No rash, edema or cyanosis.
Neurological: Alert, AAOx3, CN 2-12 grossly intact. 5/5 muscle strength (except right arm limited by pain proximally-intact distally) and sensations throughout
Labs/Imaging:
CBC: 11.37>13.3/37.7<176 65% Neutrophils, 21% Bands, 2% Lymphocytes, 8% Monocytes Blood Culture: Pending
CMP: 127/4.3 93/25 11/1.1 110/8.6 AST/ALT 44/66 ALKP 128 Alb 3.0 TPROT 6.6 TB 1.4
CPK: 170
CRP: 29.2 mg/dl (0.0-0.8)
Lactate: 1.2
Urine: Cloudy, SG 1.012, pH 6.5, LE Negative, Nitrites Negative, Protein 30, Small Blood, RBC 11-25, WBC 0-5, Urobilinogen >12.0 Urine Culture: Pending
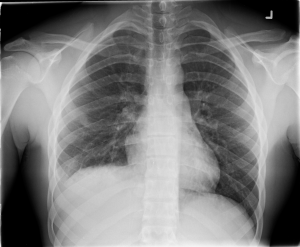
CXR as below

At this point, the patient has received IV morphine, PO ibuprofen, and a NS bolus.
His VS are HR 101, T 38, BP 122/70, Pox 98%, RR 20.
His pain score is reported at 7-8. He looks somewhat more comfortable but still has difficulty moving his right arm at the shoulder, deep breathing, and sitting up straight due to pain.
Questions for you:
How would you approach this case? Please share your opinions by clicking on “What do you think?” below.
Hmmm… RUQ pain/tenderness, +Murphy sign, +right CVA tenderness, decreased BS right base, high grade fever (104.6F), referred right shoulder/back pain without point tenderness, c/o dyspnea with orthopnea, bandemia, elevated CRP, small right sided effusion on CXR and elevated right hemidiaphragm without obvious intrapulmonary process suggests diaphragmatic irritation from RUQ infectious source (? perihepatitis, ? liver abscess, ? perinephric/retroperitoneal abscess). The “walking with a hump” is also consistent with an intra-abdominal process leading to inflammation and pain. This needs imaging. Many would start with an RUQ ultrasound, but I’d strongly consider CT with IV contrast.
Dewesh makes some useful suggestions. I am intrigued by the patient’s hyponatremia, with perhaps a R basilar process on Xray and secondary SIADH from such? Still with concentrated urine but hematuria. I’ll scratch my head, but suggest we cover pneumonia, obtain that CT (chest and abdomen) and admit for further observation. Suspect the R shoulder pain to be referred from the diaphragm from an intrathoracic process.
This is where a bedside ultrasound of the chest, RUQ/FAST could help localize any free fluid/abscess thus help direct the next best formal imaging test to look for chest vs abdomen pathology.
Bedside ultrasound is great idea Cathy. For those who need her phone number, it is 703-785-8788 and she is available 24/7. For physicians who graduated more than 5 years ago (me) or who did not do a fellowship in ultrasound (me) or who have stock in Siemens (I deny this), CT sounds like a good option that should probably be addressed before admission. I would probably head right to CT as almost any finding short of simple cholecystitis (unlikely here) will be followed up with CT.
I agree with Dewesh and it is hard to add much to this. Having said that, there is the occasional time when you get pretty severe pleuritic (or diaphragmatic) chest pain that can be the result of a pleural based process that is simply not seen on CXR.