
Ultrasound evaluation of a teenage female with abdominal pain
Posted on: April 22, 2017, by : Sam Zhao
Case:
A 15 year old girl presents to the Emergency Department for evaluation of abdominal pain. It started in the morning as generalized pain that did not radiate. It was associated with two well-formed stools, the second of which was entirely red throughout, which the patient was worried could be bloody. She denies nausea, vomiting, or diarrhea. The abdominal pain has completely resolved by the time of presentation.
Menarche was several years ago and she now has regular monthly cycles. Her LMP was completed five days prior to presentation.
ROS: Otherwise negative
PMH/PSH/FH: Unremarkable
SH: Denies sexual activity
Physical Exam:
T 36.4, HR 108, BP 105/62, RR 16, O2 sat 100% on room air
The patient is alert, well-appearing, and interactive with the physician. Her abdomen is soft, non-tender, and non-distended. Rectal exam reveals no fissures or bleeding. The rest of her examination is unremarkable.
Point-of-care ultrasound (POCUS) findings:
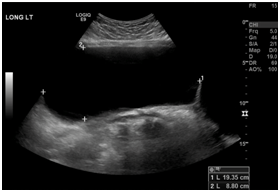
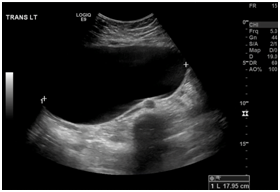
A limited transabdominal exam was performed using the Zonare C9-3 curved array probe.
Bedside interpretation: A large (approximately 12cm x 17cm x >20cm) simple cyst was found in the pelvis extending above the level of the umbilicus. There was also a small amount of pelvic free fluid seen on the sagittal view.
ED Course:
OB/GYN was consulted to work up the simple cyst. They recommended a formal ultrasound of the pelvis and likely outpatient surgical management.
Ultrasound in the radiology department findings:
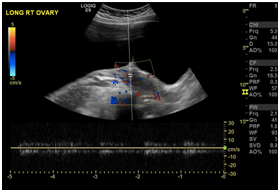

Radiology interpretation: Large (21 x 9 x 18 cm) well-marginated, anechoic structure
within the abdomen and pelvis, compatible with a cyst. No discrete internal complexity, wall nodularity or internal vascularity. Differential: mesenteric cyst, paratubal cyst, other fallopian or ovarian etiology. Normal sonographic appearance of the ovaries.
Discussion:
The patient was discharged home from the Emergency Department and brought back for elective surgical resection ten days after initial presentation. She underwent a left paratubal cystectomy via mini-laparotomy under general anesthesia. A 15cm paratubal cyst was removed and 2200cc of clear fluid was removed from the cyst. The patient tolerated the procedure well and was discharged home from the PACU. The final pathologic diagnosis was a serous cystadenoma.
Ovarian serous cystadenomas are among the most common benign ovarian neoplasms and can range in size from 5 to 20 cm. They are frequently found, as in this case, incidentally on abdominal and pelvic ultrasounds. In 2008, the International Ovarian Tumor Analysis (IOTA) group introduced the Simple Rules, which classified tumors as Benign, Malignant, or Inconclusive based on five ultrasound features typical for benign tumors (B-features) and five ultrasound features typical for malignant tumors (M-features) (1):

Several studies were conducted after the release of the Simple Rules to validate the model. An international cross-sectional cohort study involving 22 oncology centers, referral centers for ultrasonography, and general hospitals was performed that used logistic regression analysis to estimate the risk of malignancy based on the 10 ultrasound features described (2). Our patient met three of the B-rules (unilocular, presence of acoustic shadows, and no blood flow) and none of the M-rules. Only 1% of patients with this combination of features was observed to have a malignant adnexal mass on histopathologic diagnosis. Fortunately, our patient’s diagnosis correlated well with her ultrasound findings, and she has not sought further care in the Emergency Department since her surgical intervention.
1. Timmerman D, Testa AC, Bourne T, et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer. Ultrasound Obstet Gynecol 2008 Jun;31:681-90.
2. Timmerman D, Van Calster B, Testa AC, et al. Predicting the risk of malignancy in adnexal masses based on the Simple Rules from the International Ovarian Tumor Analysis group. Am J Obstet Gynecol 2016 Apr;214:424-437.