
Ultrasound evaluation of infant with scrotal swelling
Posted on: February 1, 2017, by : Caleb Ward MD
Case:
A 3-month-old male was referred to the ED by his PCP for concern over left scrotal swelling. Parents reported one month of seemingly non-tender swelling without overlying skin changes. He was feeding well and gaining weight. There had been no work-up.
PMHx: Full term vaginal delivery, received usual prenatal care.
Exam:
Vitals: weight 9.9kg, temp 36.1, heart rate 108, respiratory rate 28, SpO2 100% (RA)
Gen: Alert, chubby baby, smiles, no distress
GU: Tanner 1 external genitalia, not circumcised, left testicle appears larger than right and is firm, mildly tender with a symmetric cremasteric reflex
The remainder of his exam is within normal limits.
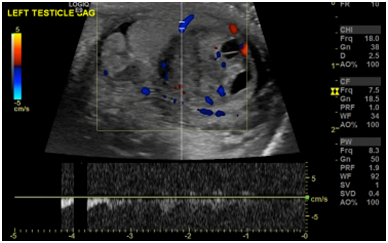
Point-of-care ultrasound (POCUS) findings (linear transducer):
Bedside interpretation: Left testicle had heterogeneous appearance with cystic elements and was larger than the contralateral testicle. There appeared to be pulsatile flow (images not included). Suspicion was for testicular tumor.
Ultrasound in the radiology department findings:



Radiology interpretation: heterogeneous mixed cystic solid vascular well circumscribed mass within the left testis measuring 1.4 X 1.4 x 1.5cm. Rule out germ cell tumor such as yolk sac or teratoma. Juvenile granulosa cell tumor is another possibility. Testis has normal vascularity.
Plan:
Urology and Oncology consults were placed. Screening labs were notable for WBC 19.5K/mcL. Specific follow up labs were all normal including: LDH 369 units/L, uric acid 2.3 mg/dL, AFP 247 iu/mL and serum HCG 1 mIu/mL. He was discharged home and returned for unilateral orchiectomy 3 days alter. Surgical pathology revealed a 1.3cm juvenile granulosa cell tumor with margins free of tumor.
Discussion:
The patient was ultimately diagnosed with a juvenile granulosa cell tumor (JGCT). A case series of 70 JGCTs found that 90% of cases were aged less than 6 months, with the most common presentation being with a testicular mass (1). Approximately 2/3 of these cases had a cystic component with the remainder entirely solid. This is typically a benign entity with an excellent prognosis. Orchiectomy is the definitive management, though given the benign clinical course, testis-sparing surgery when technically feasible may be considered.
Marin et al in their recent summary of the evidence for pediatric emergency medicine POCUS (2) note that there is a single retrospective study of POCUS performed by emergency physicians on 36 adults with acute testicular pain. ED physicians diagnosed multiple testicular entities with a sensitivity of 95% and specificity of 94% (3). There were no cases of missed testicular torsion. The use of POCUS by PEM physicians in pediatric patients has thus far not been studied other than in isolated case reports (4,5,6).
1. Kao CS, Cornejo KM, Ulbright TM et al. Juvenile granulosa cell tumors of the testis: a clinicopathologic study of 70 cases with emphasis on its wide morphologic spectrum. Am J Surg Pathol. 2015;39(9):1159-69.
2. Marin JR, Abo AM, Arroyo AC et al. Pediatric emergency medicine point-of-care ultrasound: summary of the evidence. Crit Ultrasound J. 2016;8(1):16.
3. Blaivas M, Sierzenski P, Lambert M. Emergency evaluation of patients presenting with acute scrotum using bedside ultrasonography. Acad Emerg Med. 2001;8(1):90-3.
4. Blaivas M, Batts M, Lambert M. Ultrasonographic diagnosis of testicular torsion by emergency physicians. Am J Emerg Med. 2000;18(2):198-200.
5. Thimann D, Badawy M. 7-month-old male with scrotal swelling. Emerg Med J. 2014;31(6):521-2.
6. Matzek BA, Linklater DR. Traumatic testicular dislocation after minor trauma in a pediatric patient. J Emerg Med. 2013;45(4):537-40.